Medications
Pharmacologic options for myofascial pain — what the evidence does and does not support.
Treatment
Medications for Myofascial Pain
Complete pharmacology guide — from OTC analgesics to adjuvant medications. Understand mechanisms, dosing, and evidence before your appointment.
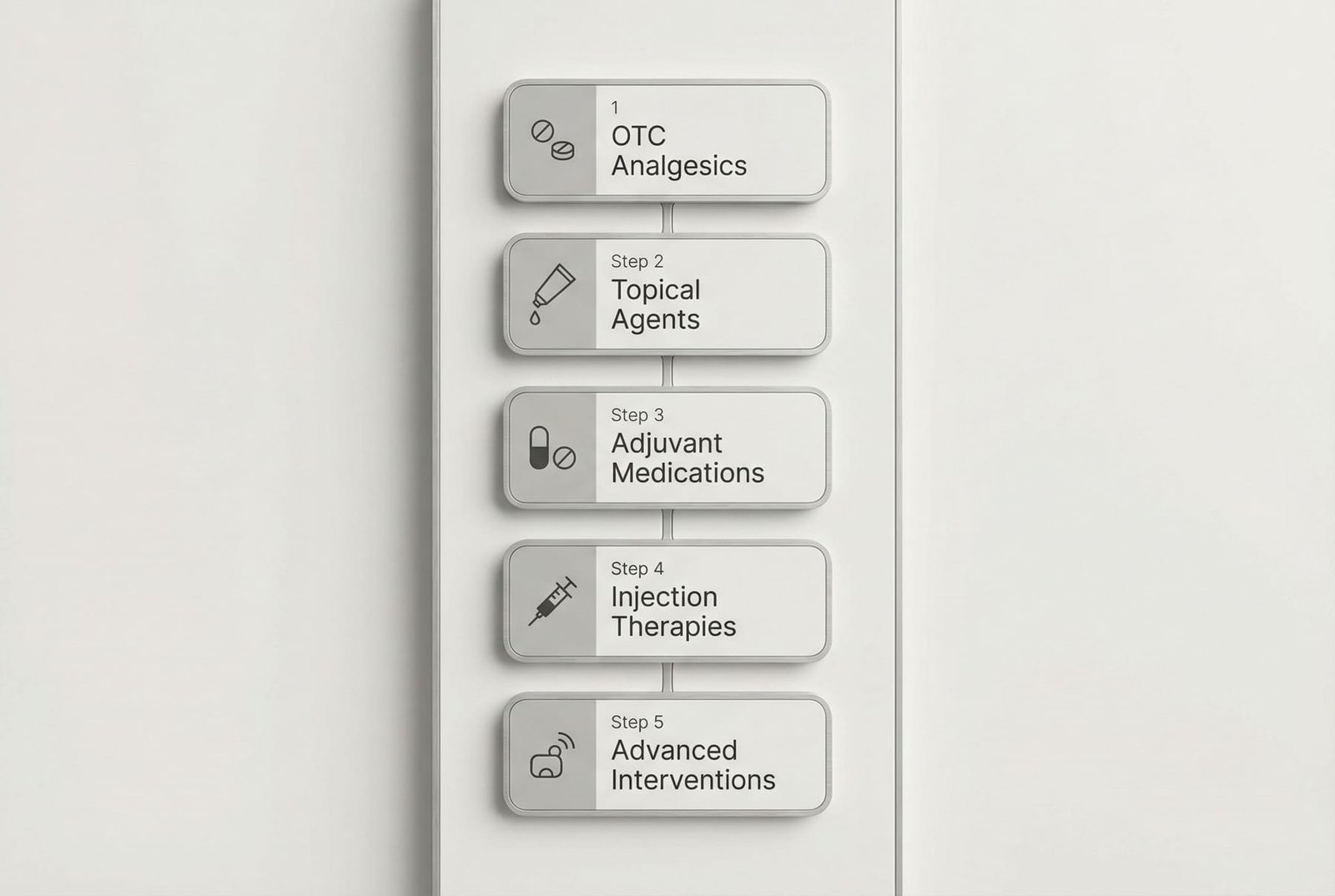
Medications & Pharmacology
Complete overview of OTC, prescription, adjuvant, and injection therapies. Pharmacological hierarchy and why opioids fail.

Supplements & Nutrition
Evidence-based supplements — magnesium, vitamin D, CoQ10, omega-3s — anti-inflammatory diets, and nutritional strategies for myofascial pain.
Treatment Errors to Avoid
Common mistakes patients and practitioners make that worsen trigger points or prevent recovery.

NSAIDs
Ibuprofen, naproxen, diclofenac, celecoxib — COX inhibition, topical vs oral, GI/CV/renal risks, and practical prescribing for myofascial pain.
Non-Opioid Analgesics
Acetaminophen and Dipyrone (Metamizole). Mechanisms, dosing, hepatotoxicity, agranulocytosis debate, and combination products.
Muscle Relaxants
Cyclobenzaprine, tizanidine, methocarbamol, orphenadrine, baclofen. Central mechanisms, individual profiles, and short-term use guidelines.

Capsaicin (Topical)
TRPV1 receptor desensitization, substance P depletion, OTC creams vs Qutenza 8% patch, and how to use effectively for trigger points.
Topical Lidocaine
Lidoderm 5% patch, creams, EMLA. Sodium channel blockade, clinical evidence, and application guide for myofascial trigger points.
TCAs (Amitriptyline-like)
Amitriptyline, nortriptyline, desipramine. Dual neurotransmitter reuptake, sodium channel blockade, NMDA antagonism — gold standard adjuvant.

SNRIs (Duloxetine-like)
Duloxetine, venlafaxine, milnacipran. FDA-approved for chronic pain. Central sensitization targeting and descending inhibition enhancement.

Gabapentinoids
Gabapentin and pregabalin. Alpha-2-delta calcium channel ligands. Wind-up reduction, central sensitization, and when to use for myofascial pain.

Opioids: Why They Fail
Why opioids are ineffective and harmful for myofascial pain. Wrong mechanism, hyperalgesia, guideline recommendations, and better alternatives.
CBD (Cannabidiol)
Non-psychoactive cannabinoid acting via FAAH inhibition, TRPV1 agonism, adenosine reuptake, and anti-inflammatory pathways. Topical, sublingual, and oral formulations.

Corticosteroids
The most injected anti-inflammatory class. Triamcinolone, dexamethasone, methylprednisolone — PLA2 inhibition, NF-κB suppression, and use-limited protocols.

Low-Dose Naltrexone (LDN)
Off-label opioid antagonist paradox: TLR4 antagonism, microglial M1→M2 shift, endogenous opioid rebound. Unique mechanism at 1-4.5mg dosing.
Vitamin B Complex for Neuropathic Pain
B1, B6, B12 mechanisms for nerve repair and pain modulation — complete clinical guide.
Topical Compounding Formulations
Custom transdermal medications — ketoprofen, baclofen, gabapentin, cyclobenzaprine in PLO gel. High-concentration local delivery with minimal systemic side effects.
Tizanidine vs. Muscle Relaxants
Practical comparison guide — why tizanidine is preferred for MPS, cyclobenzaprine's 18h half-life problem, and why carisoprodol should be avoided.
Medical Cannabis for Myofascial Pain
Beyond CBD — THC:CBD ratios, endocannabinoid system, routes of administration, opioid-sparing evidence, and practical clinical guide.
Neuroleptics for Refractory MPS
Chlorpromazine (Amplictil), levomepromazine (Neozine), quetiapine — D2 blockade for treatment-resistant pain, sedation as a tool, and cautious off-label use in refractory cases.

Benzodiazepines — Why Not Recommended
GABA-A agonists that mask symptoms without treating trigger points. High dependence risk, impaired motor learning, and why safer alternatives exist.
Sleep Architecture Modulators
Trazodone, Z-drugs (zolpidem, eszopiclone), and suvorexant — restoring Stage 3/4 NREM sleep as a treatment strategy for chronic MPS.
Alpha-2 Adrenergic Agonists
Clonidine, tizanidine, and dexmedetomidine — central sympatholytic agents that reduce sympathetic hyperactivity maintaining trigger points.
Magnesium for Myofascial Pain
Glycinate, malate, and threonate forms — physiological muscle relaxant, NMDA antagonist, and calcium regulator. 50-80% of population deficient.