Understanding Piriformis Syndrome
Piriformis
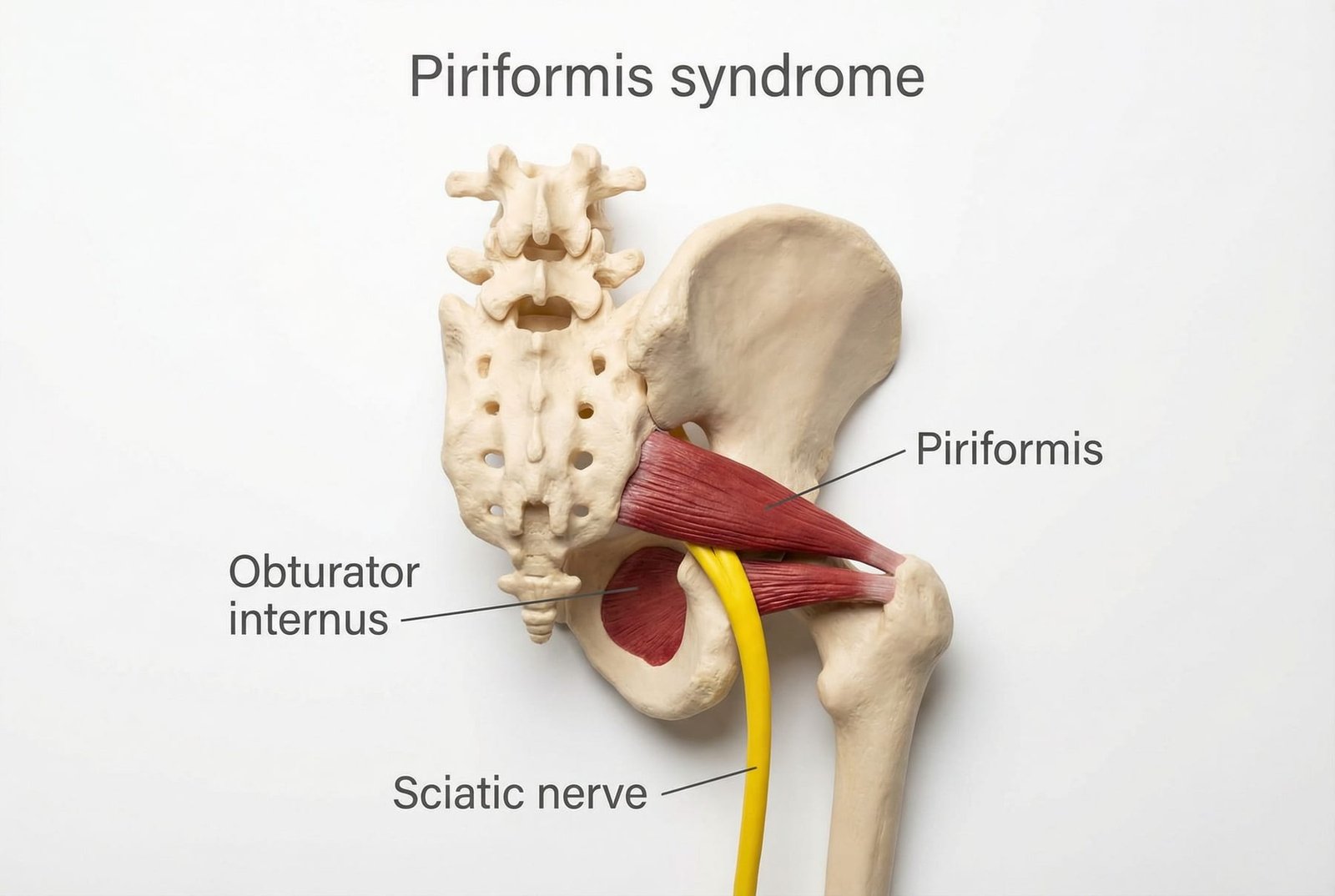
Anatomy and Pain Pattern OverviewThe piriformis is a small deep hip muscle that helps with external rotation and contributes to pelvic and hip stability. Because it lies close to the sciatic nerve, irritation in this region can sometimes create pain patterns that resemble sciatica.
In some people, the sciatic nerve and piriformis have anatomical relationships that may make the region more sensitive to compression or irritation. That said, anatomy alone does not diagnose the syndrome — the full clinical picture still matters.
Piriformis syndrome is best thought of as one member of the broader “deep gluteal pain” family. Buttock pain with leg referral can also come from the lumbar spine, gluteus minimus, gluteus medius, quadratus lumborum, hamstrings, SI region, or other neural structures.
The clinical challenge is that piriformis-related symptoms and true lumbar radicular symptoms can look similar. Good assessment focuses on pain behavior, movement provocation, neural signs, and how the hip and lumbopelvic region behave together.
Anatomy & Trigger Points
The piriformis does not act in isolation. Deep gluteal pain often involves multiple hip and trunk stabilizers that either overload together or compensate for one another.

Piriformis
Deep buttock pain with possible referral down the posterior thigh and sometimes below the knee. In some patients this can resemble sciatica, especially when sitting aggravates symptoms.
Can contribute to posterior-lateral hip pain and pseudo-sciatic referral patterns that overlap with piriformis-related symptoms.
May contribute to posterior iliac crest, sacral, or lateral hip pain and often coexists with piriformis overload when pelvic control is poor.
May add low-back, iliac crest, or greater trochanter pain that blends with deep gluteal complaints and alters pelvic mechanics.
Can contribute to deep pelvic, gluteal, or coccygeal discomfort and is often overlooked when piriformis syndrome is assumed to be the only deep hip driver.
Referral Patterns
The classic complaint is deep buttock pain with referral into the posterior thigh, especially during prolonged sitting or hip rotation positions.
Some patients also report tingling, calf discomfort, or foot symptoms. These features make the condition easy to confuse with lumbar or peripheral nerve pain, which is why neuro exam findings matter.
Piriformis syndrome matters clinically because a small deep hip muscle can create a very large and misleading symptom pattern.
Deep Buttock
Posterior Thigh
Sitting Worse
Self-Assessment Tests
No single test confirms piriformis syndrome. Clinical confidence usually comes from a combination of provocative hip tests, gluteal tenderness, symptom behavior, and exclusion of more serious spinal or neurological causes.
FAIR Test
Pace Sign
Freiberg Test
Beatty Test
Treatment Pathways
Treatment usually starts conservatively and progresses only if symptoms, function, and diagnostic certainty justify doing more.

Treatment Pathways
Mechanism DiagramSelf-Care
A reasonable first step for mild to moderate symptoms, especially when prolonged sitting, hip stiffness, or gluteal tightness are the main aggravators.
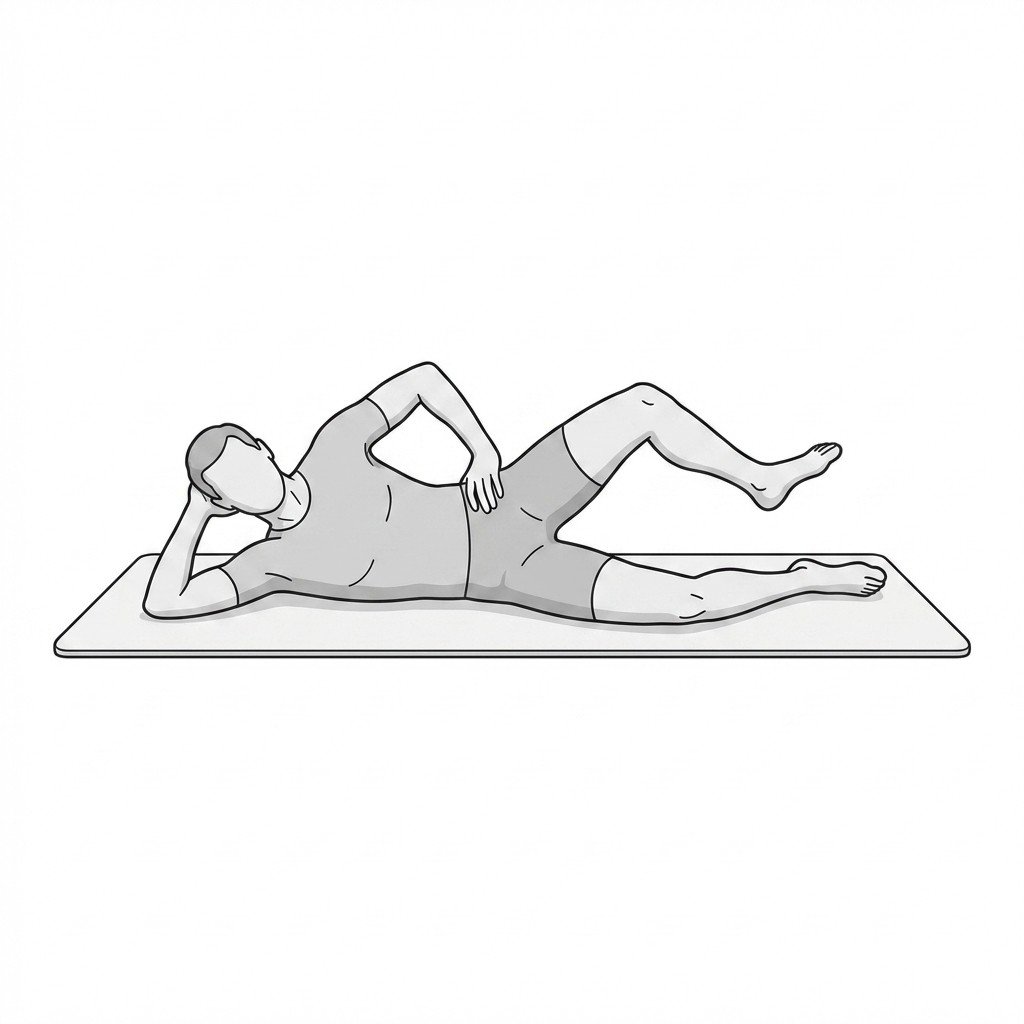
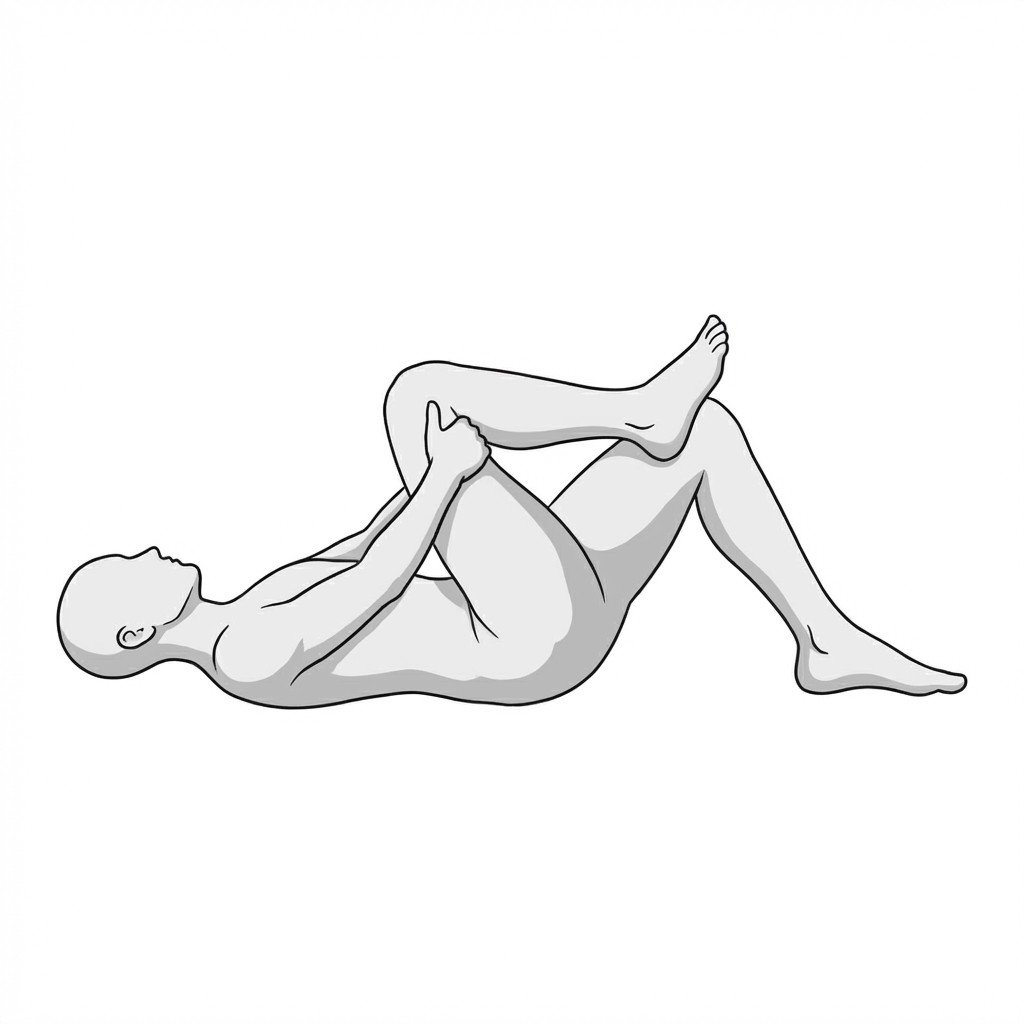
- Gentle figure-4 style stretching if it reduces symptoms rather than increases them
- Modified gluteal or piriformis self-release using tolerable pressure only
- Walking breaks and reduced prolonged sitting
- Temporary avoidance of clearly provoking seated or rotation-heavy positions
- Hip mobility and breathing work to reduce guarding
Manual Therapy
Hands-on care may help when deep gluteal muscles are hard to access independently or when there is broader lumbopelvic stiffness contributing to the problem.
- Myofascial treatment of the deep lateral rotator region
- Post-isometric relaxation or other clinician-guided lengthening strategies
- Adjacent hip, SI, or lumbopelvic assessment when relevant
- Treatment of coexisting gluteal, QL, or hip-flexor contributors
- Progression into movement rather than passive care alone
Interventional
Targeted procedures may be considered in selected cases when conservative care is not enough and the diagnosis is reasonably clear.
- Dry needling in experienced hands
- Trigger point injection in selected refractory cases
- Image-guided procedures when anatomy or depth makes blind treatment less appropriate
- Nerve-focused procedures only when the neural component is a real diagnostic or therapeutic target
Rehabilitation
Long-term improvement usually depends on correcting the movement and loading problems that keep the piriformis region overloaded.
- Hip abductor and external rotator strengthening
- Core and lumbopelvic control work
- Gradual return to running, lifting, or sport-specific movement
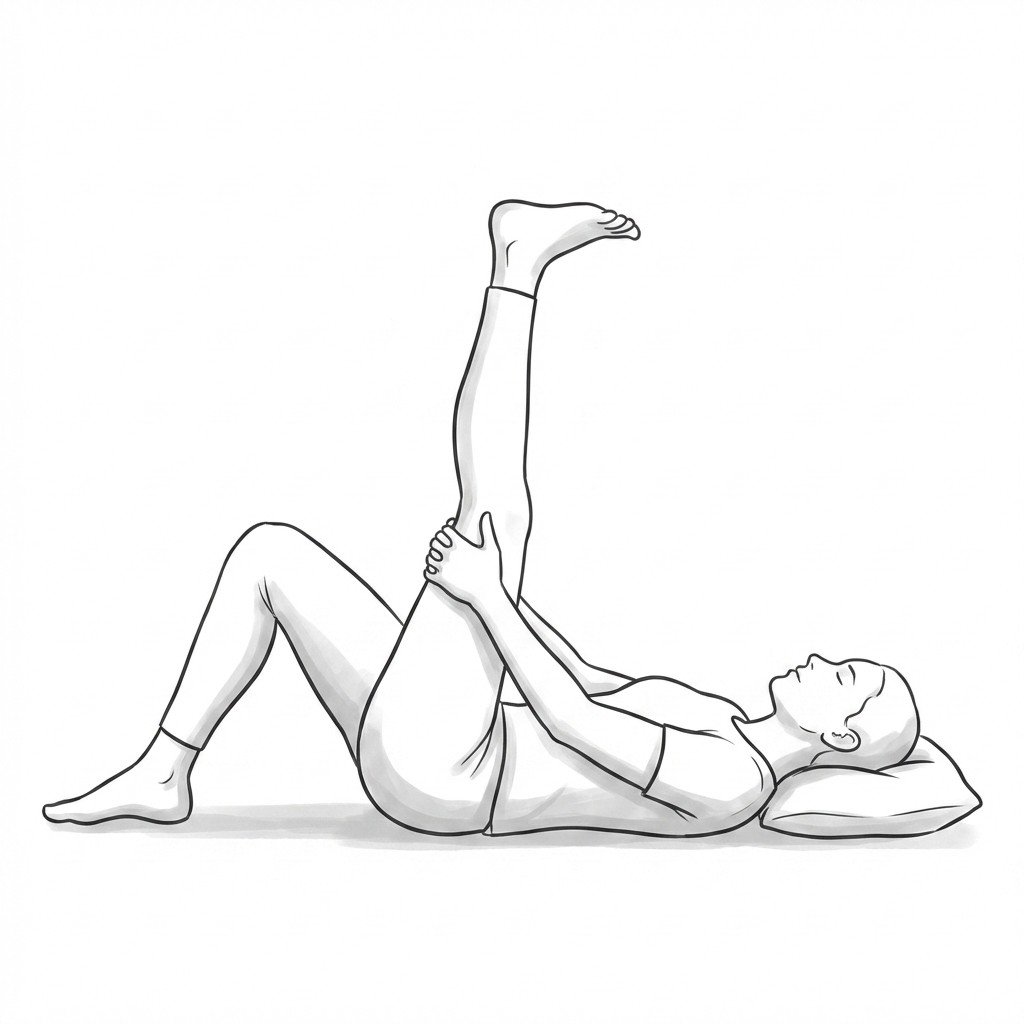
- Neural mobility work in selected cases
- Ergonomic and sitting-position modification when prolonged sitting is a trigger
Red Flags — When to See a Doctor
Deep buttock pain with leg symptoms can come from serious spinal or systemic causes. The following features should prompt medical review rather than routine self-treatment.
Piriformis syndrome is one possible cause of deep buttock pain and sciatic-like symptoms, but it is not the only one.
The condition is most convincing when hip-position tests, buttock palpation, and symptom behavior all point toward a deep gluteal source rather than a spinal one.
The piriformis is only one part of the deep gluteal picture — gluteal muscles, obturator internus, QL, and lumbopelvic mechanics often matter too.
Most treatment plans start conservatively with stretching, load modification, and hip rehabilitation before escalating.
Red flags such as progressive weakness, bowel or bladder changes, bilateral symptoms, or systemic features require prompt medical review.
Movement therapy
Exercises for Piriformis Syndrome
Piriformis syndrome requires both stretching the external rotators and reloading hip abduction so the piriformis stops being overworked as a compensator. Start with 2–3 and progress as tolerated.