Interventional
Trigger-point injections, botulinum toxin, and other procedural options.
Treatment
Interventional Treatments
Needle-based, injection, and device therapies — from dry needling to shockwave therapy. What each procedure does, its evidence, and what to expect.

HILT vs LLLT — Comparison Dashboard
Sortable, filterable comparison of HILT (iLux Smart, Hiro, K-Laser, LightForce) and LLLT platforms (THOR, MR4, BioFlex, Erchonia) — power, wavelength, penetration, dose, and RCT outcomes for musculoskeletal pain.
Dry Needling
How filiform needles target trigger points to elicit local twitch responses. Techniques, mechanisms, evidence, and what to expect.

Acupuncture for Myofascial Pain
Traditional and Western medical acupuncture for myofascial pain. Mechanisms, point selection, evidence from clinical trials.
Trigger Point Injections
Lidocaine, procaine, and saline injections directly into trigger points. Protocols, comparisons, and clinical outcomes.
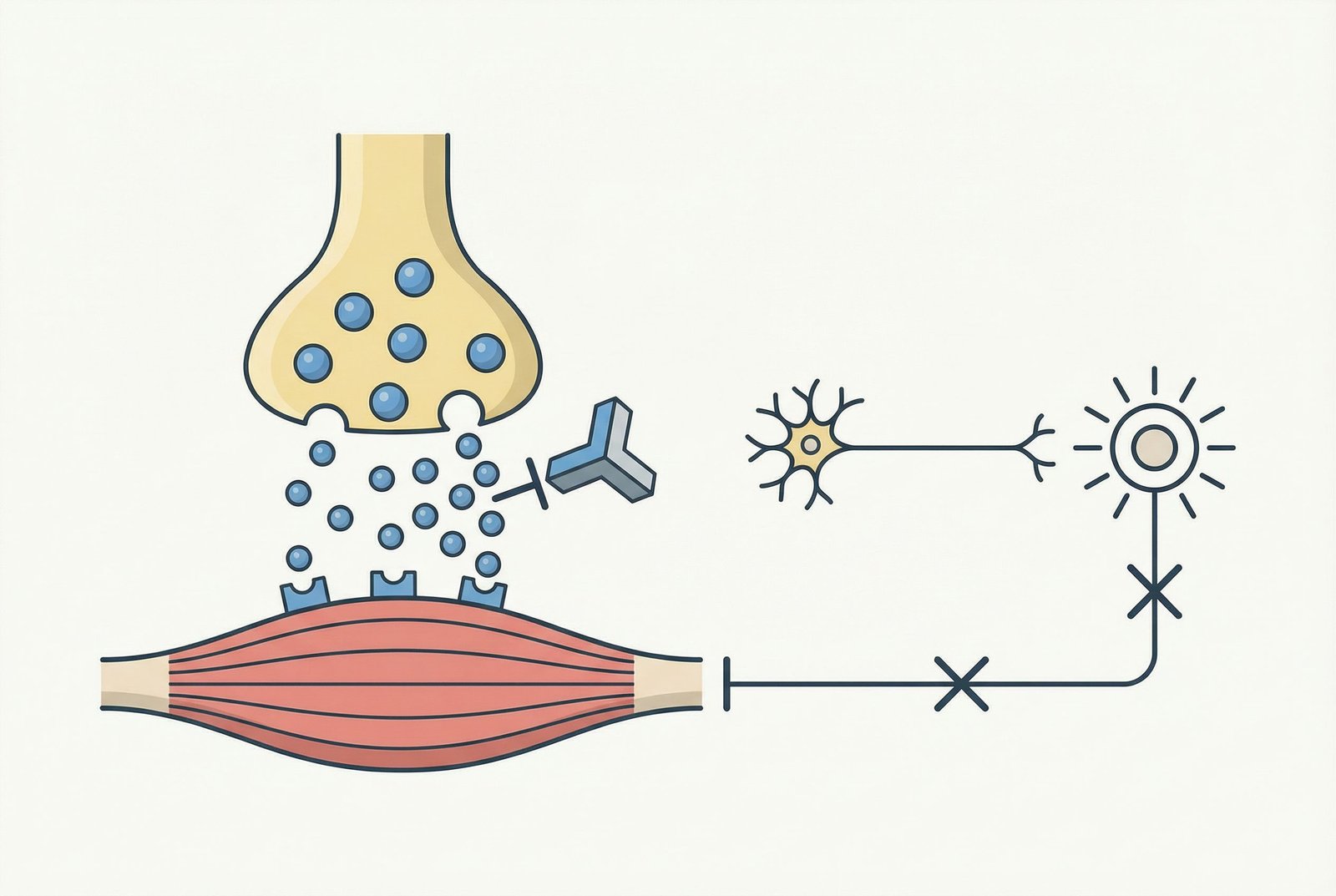
BOTOX for Trigger Points
Botulinum toxin for chronic, refractory myofascial pain. Mechanism, dosing, evidence, ideal candidates, and cost considerations.
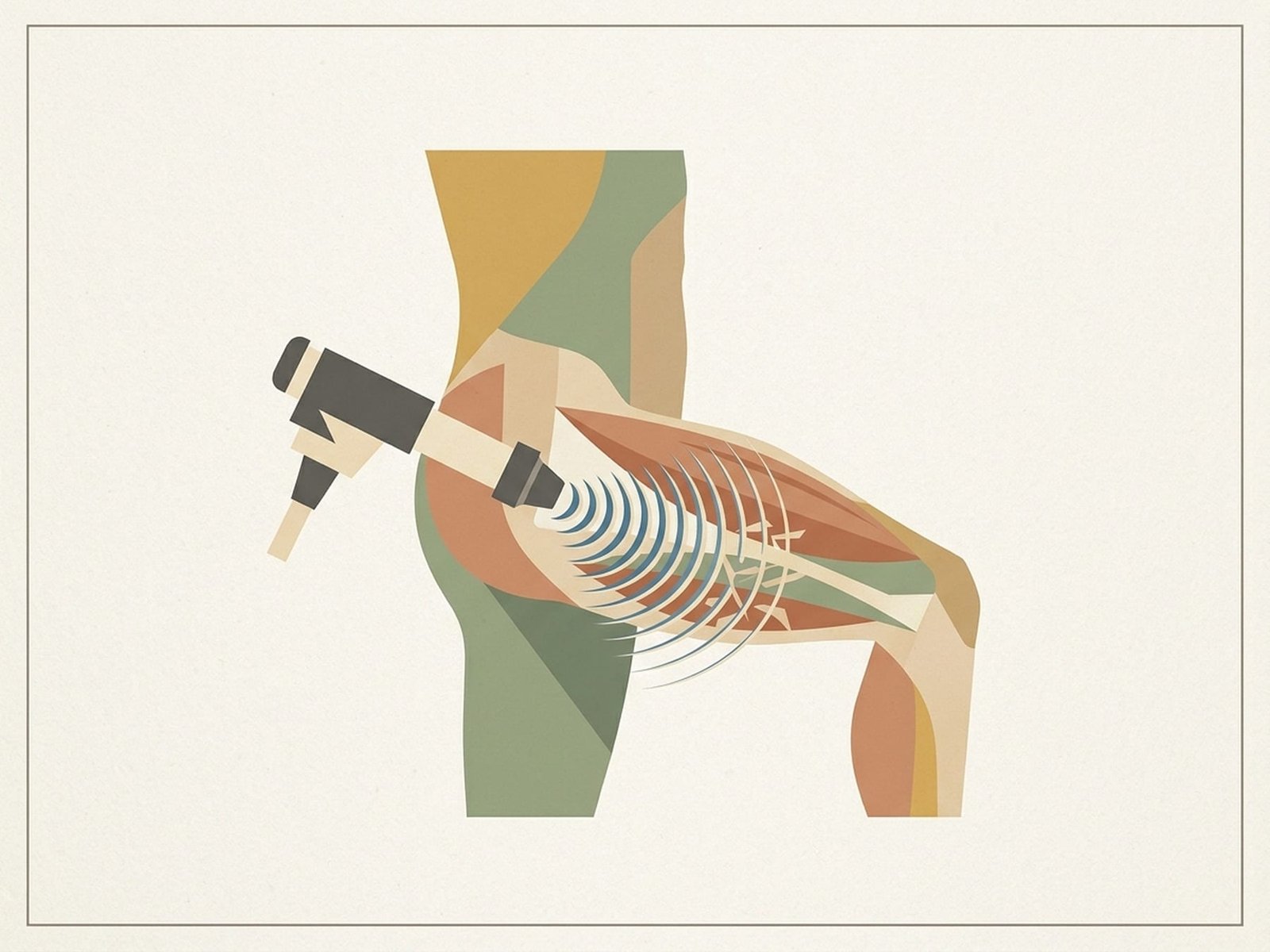
Shockwave Therapy (ESWT)
Focused and radial extracorporeal shockwave therapy for trigger points. Non-invasive, 78-85% success rate, and growing evidence base.
PENS — Deep Electrical Stimulation
Percutaneous electrical nerve stimulation — needle electrodes delivering current past skin impedance for 10-100× more efficient stimulation than TENS.
Electroacupuncture
Electrical stimulation through acupuncture needles. Frequency-dependent opioid release, standardized dosing, and enhanced analgesia for myofascial pain.
PRP (Platelet-Rich Plasma)
Autologous platelet-rich plasma injections for trigger points. Growth factors, tissue regeneration, and emerging evidence for refractory myofascial pain.

Mesotherapy
French intradermal microinjection technique. Multi-agent cocktails (procaine, piroxicam, B12) targeting pain at the source — peu, rarement, au bon endroit.

Prolotherapy
Regenerative injection therapy with hypertonic dextrose. Controlled inflammation triggers collagen synthesis, fibroblast proliferation, and tissue repair.
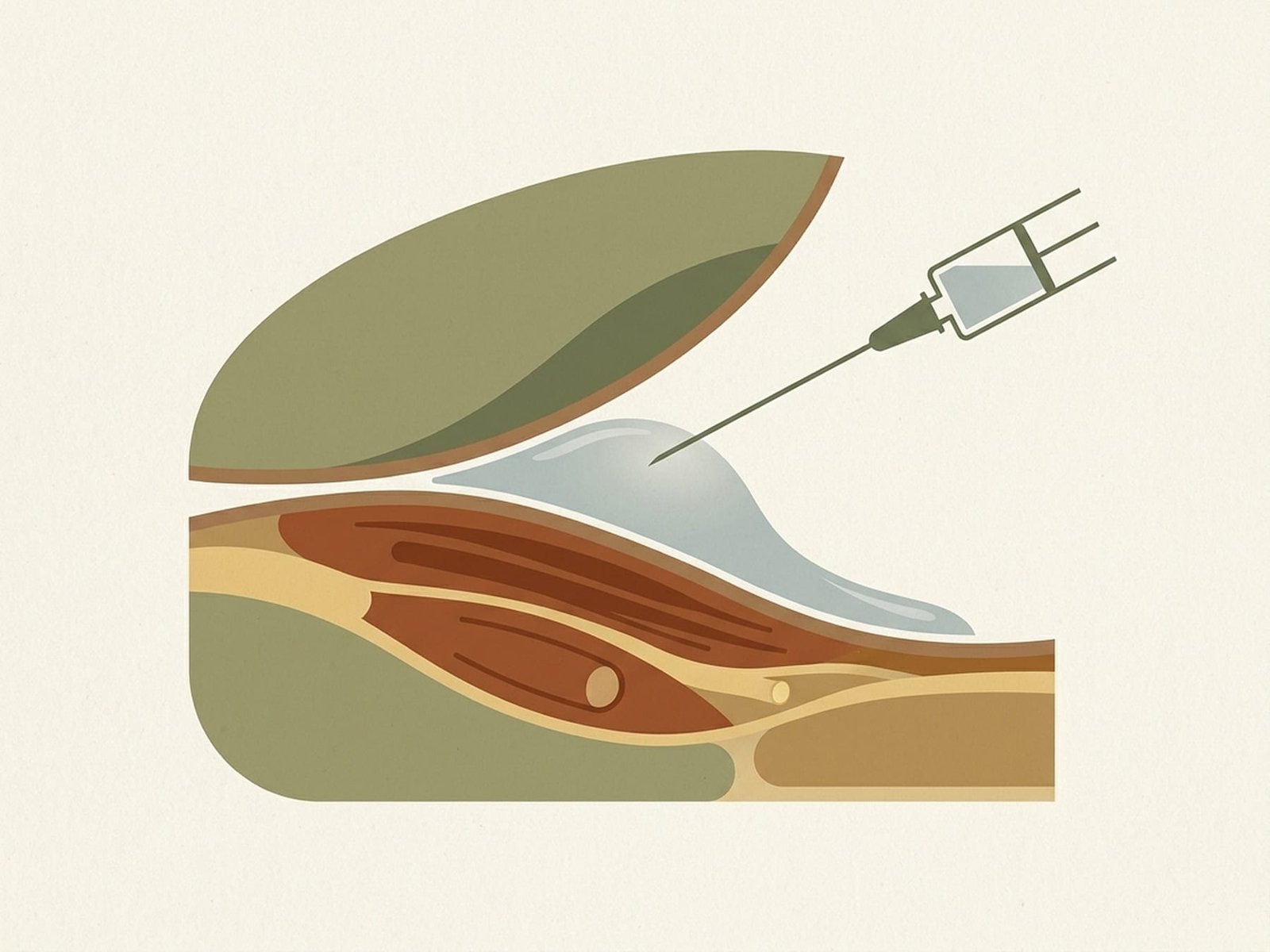
Saline Hydrodissection
Ultrasound-guided tissue plane separation for fascial adhesions and nerve entrapment — cluneal, dorsal scapular, spinal accessory nerve liberation.

Cupping Therapy (Ventosa)
Myofascial decompression through negative pressure — wet, dry, and sliding cupping for trigger point release.
Ketamine for Refractory MPS
NMDA receptor blockade and central sensitization reversal — sub-anesthetic IV, intranasal, and oral ketamine protocols for treatment-resistant myofascial pain.

IASTM: Instrument-Assisted Soft Tissue Mobilization
Graston, HawkGrips, and FAKTR protocols — fibroblast activation science, region-specific applications, and a comparison with manual soft tissue therapy.

Intramuscular Stimulation (IMS)
Chan Gunn's neuropathic model for treating chronic myofascial pain through deep intramuscular needle stimulation — with comparison to dry needling approaches.

Regenerative Injection Therapies
Prolotherapy, platelet-rich plasma (PRP), and stem cell therapies compared — current evidence, appropriate patient selection, cost realities, and the future of regenerative medicine for MPS.
High-Intensity Laser Therapy (HILT)
Class IV Nd:YAG laser (1064nm, 6-12W) for deep tissue trigger point deactivation. Photobiomodulation, thermal gradients, and 60-80% pain reduction in 4-6 sessions.
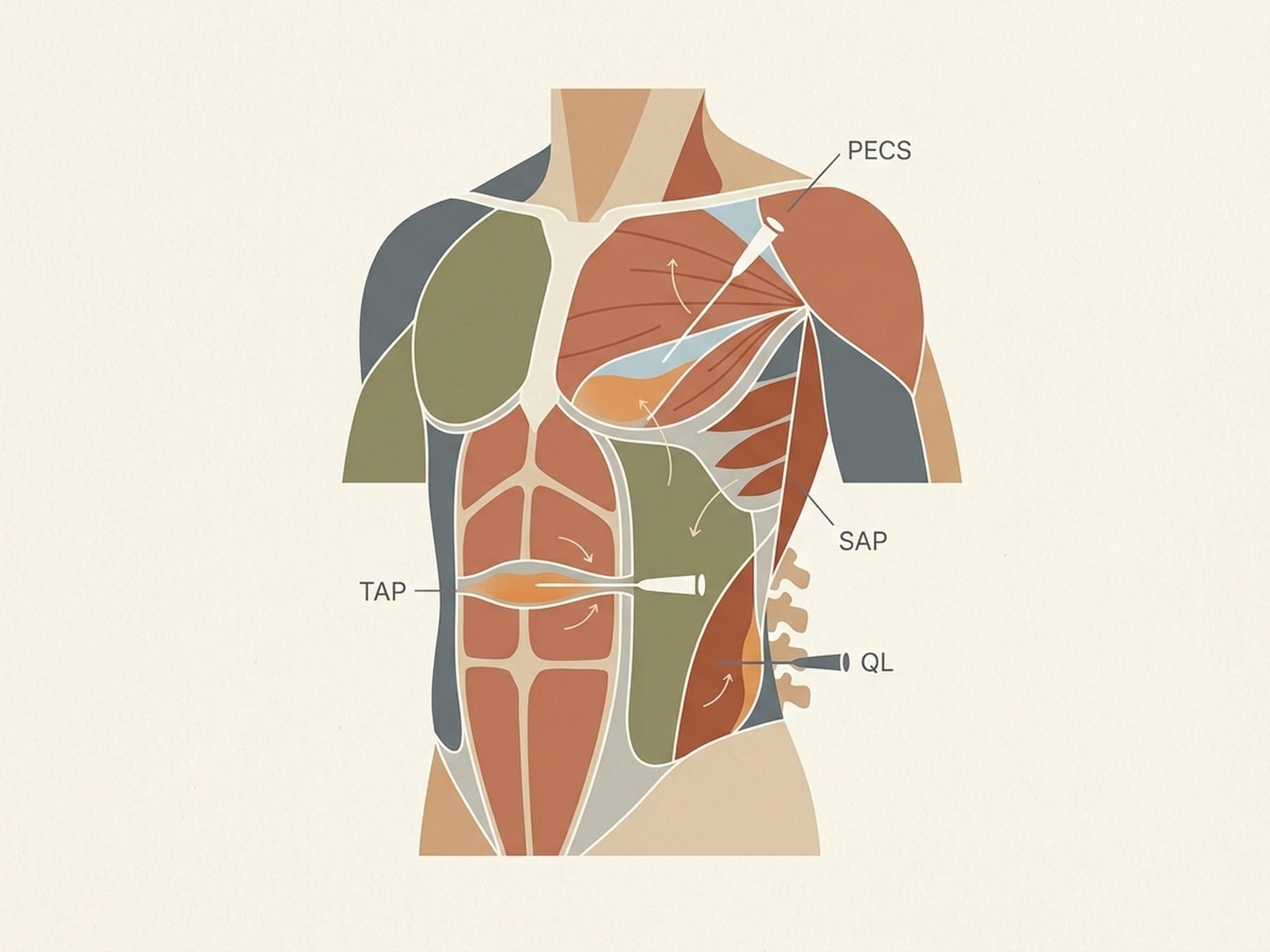
Fascial Plane Blocks
Ultrasound-guided regional anesthesia targeting fascial compartments — ESP blocks, Pecs I/II, serratus anterior plane, and QL blocks for refractory myofascial pain.

Peripheral Nerve Blocks
Targeted neural blockade for diagnostic and therapeutic management — greater occipital, suprascapular, intercostal, and sciatic blocks when MPS coexists with nerve entrapment.

TECAR Therapy
Capacitive and resistive electric transfer (448 kHz) for endogenous deep tissue heating. Reaches 3-4 cm depth with 4-7°C temperature increase for trigger point deactivation.
IV Lidocaine Infusions
Systemic sodium channel blockade for widespread, centrally sensitized myofascial pain. 1-5 mg/kg/hr over 1-4 hours with cardiac monitoring — 40-60% pain reduction.