सीखें
स्थितियों, चिकित्साओं और स्व-देखभाल पर 176 लेख — सभी प्रमाण की मज़बूती के आधार पर श्रेणीबद्ध। बुनियादी बातों से शुरुआत करें, या सीधे उस विषय पर जाएँ जिसका आप इलाज कर रहे हैं।
यहाँ से शुरू करें
शुरुआती गाइड
अगर आप ट्रिगर पॉइंट थेरेपी से नए परिचित हैं, तो पहले पढ़ने लायक पाँच चीज़ें। मरीज़ों के लिए ख़ास तौर पर तैयार किया गया एक चरणबद्ध रास्ता।
पढ़ें →अक्सर पूछे जाने वाले सवाल
मायोफेशियल दर्द, स्व-उपचार और डॉक्टर से कब मिलें — इन पर सबसे आम सवालों के सीधे जवाब।
पढ़ें →कहाँ से शुरू करूँ?
पहले क्या पढ़ें, यह तय नहीं कर पा रहे? कुछ सवालों के जवाब दीजिए और अपने लिए ख़ास पढ़ाई का रास्ता पाइए।
पढ़ें →विषय के अनुसार ब्राउज़ करें
स्थितियाँ और निदान
चिकित्साएँ
स्व-देखभाल
दवाएँ
शोध पुस्तकालय
व्यायाम पुस्तकालय
विशेष लेख
सभी विषय
176 लेखGetting Started
New here? These guides will orient you — no jargon, no overwhelm, just the essentials.
Answer 3 simple questions and get a personalized path to exactly what you need — whether you're in pain, newly diagnosed, or helping a loved one.
Your first 5 essential reads, a week-one plan, and reassurance that this IS real, treatable, and you're not alone.
Plain-language definitions for 100+ terms — from "taut band" to "central sensitization." Searchable and filterable.
Losing the life you had and finding a way forward — the 5 stages of grief adapted for chronic pain, validation, and practical coping at each stage.
Common Pain Patterns
Dedicated guides for the most common myofascial pain presentations — anatomy, self-tests, and treatment pathways.
How cervical and cranial trigger points create band-like headache patterns — and how to break the cycle.
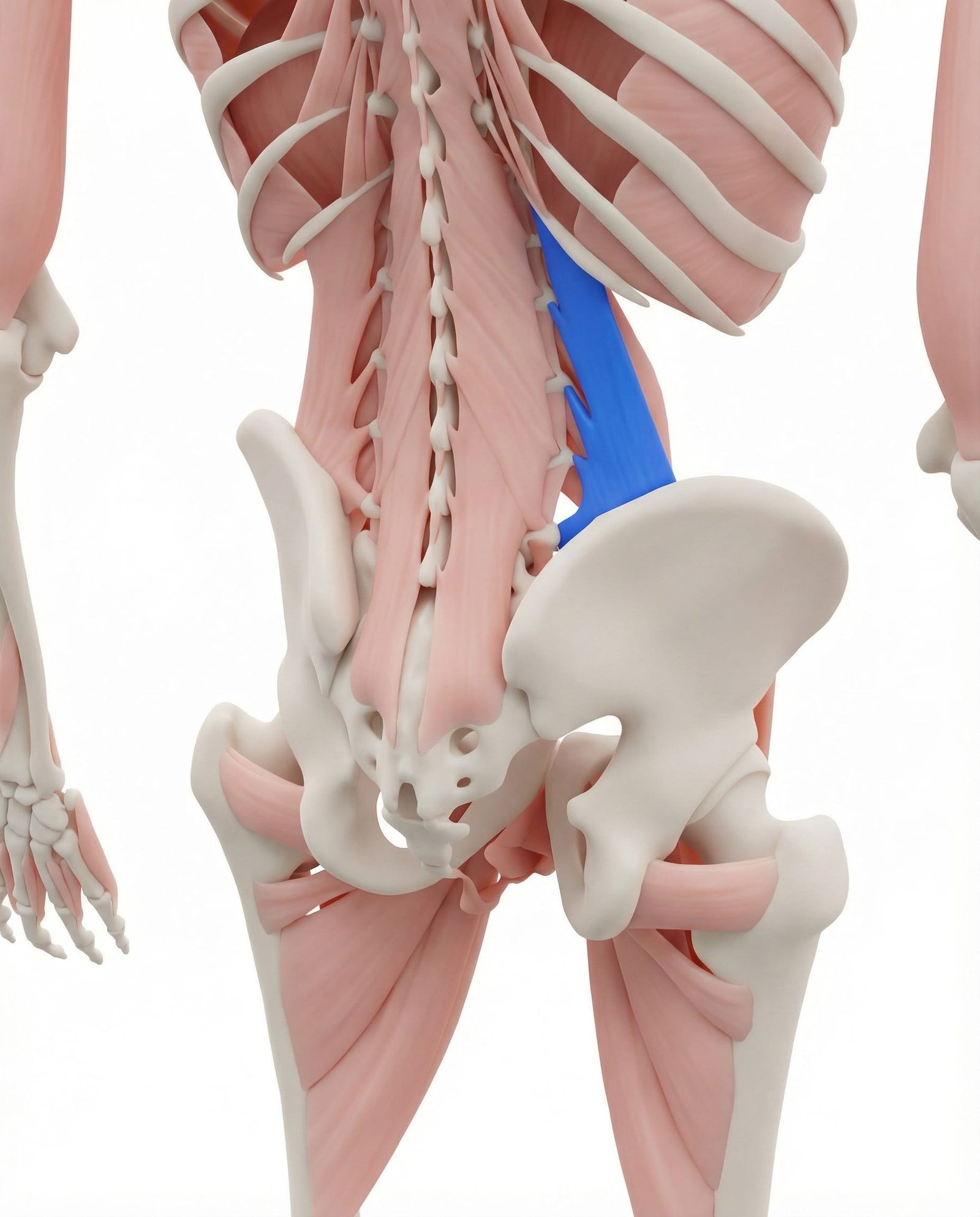
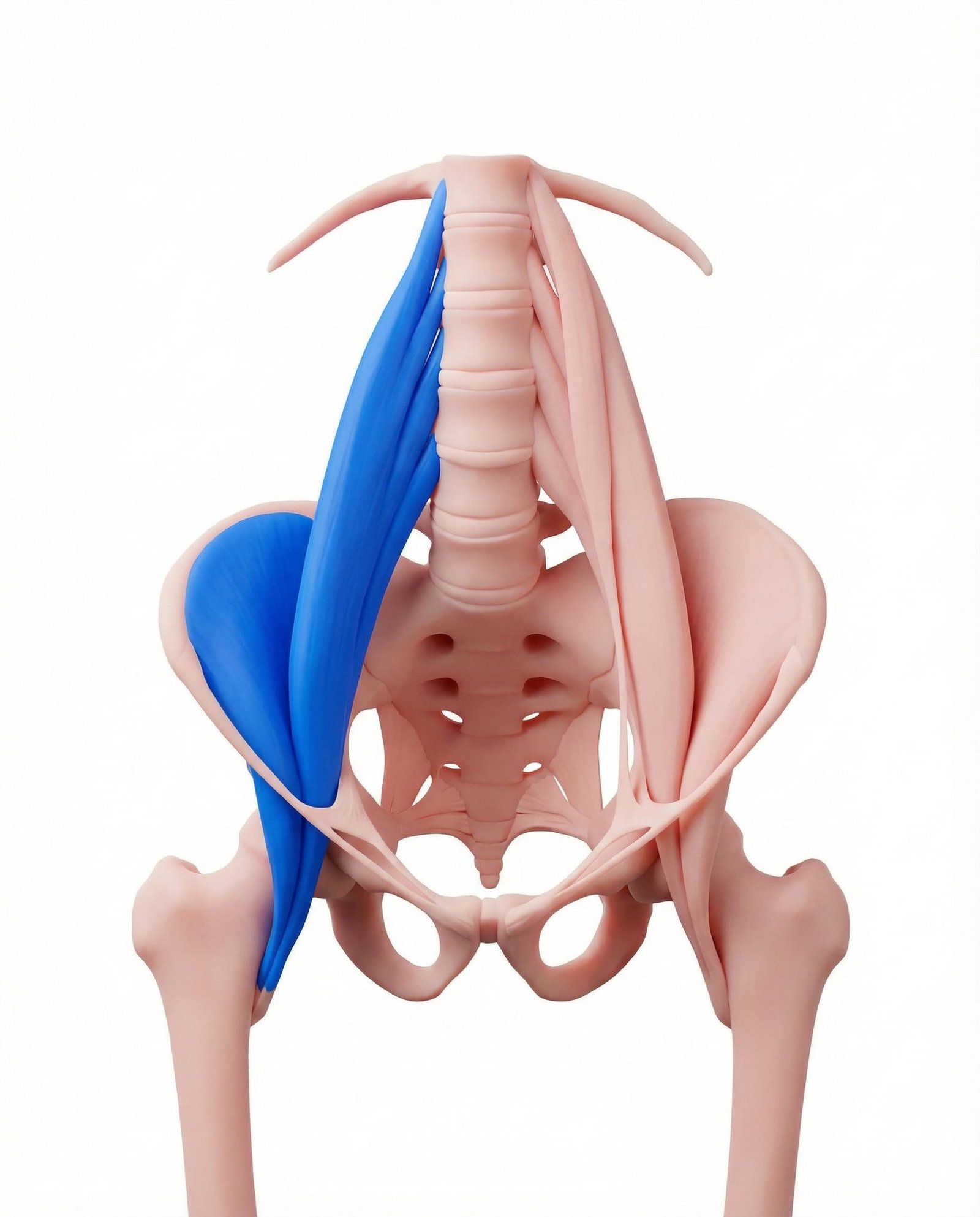
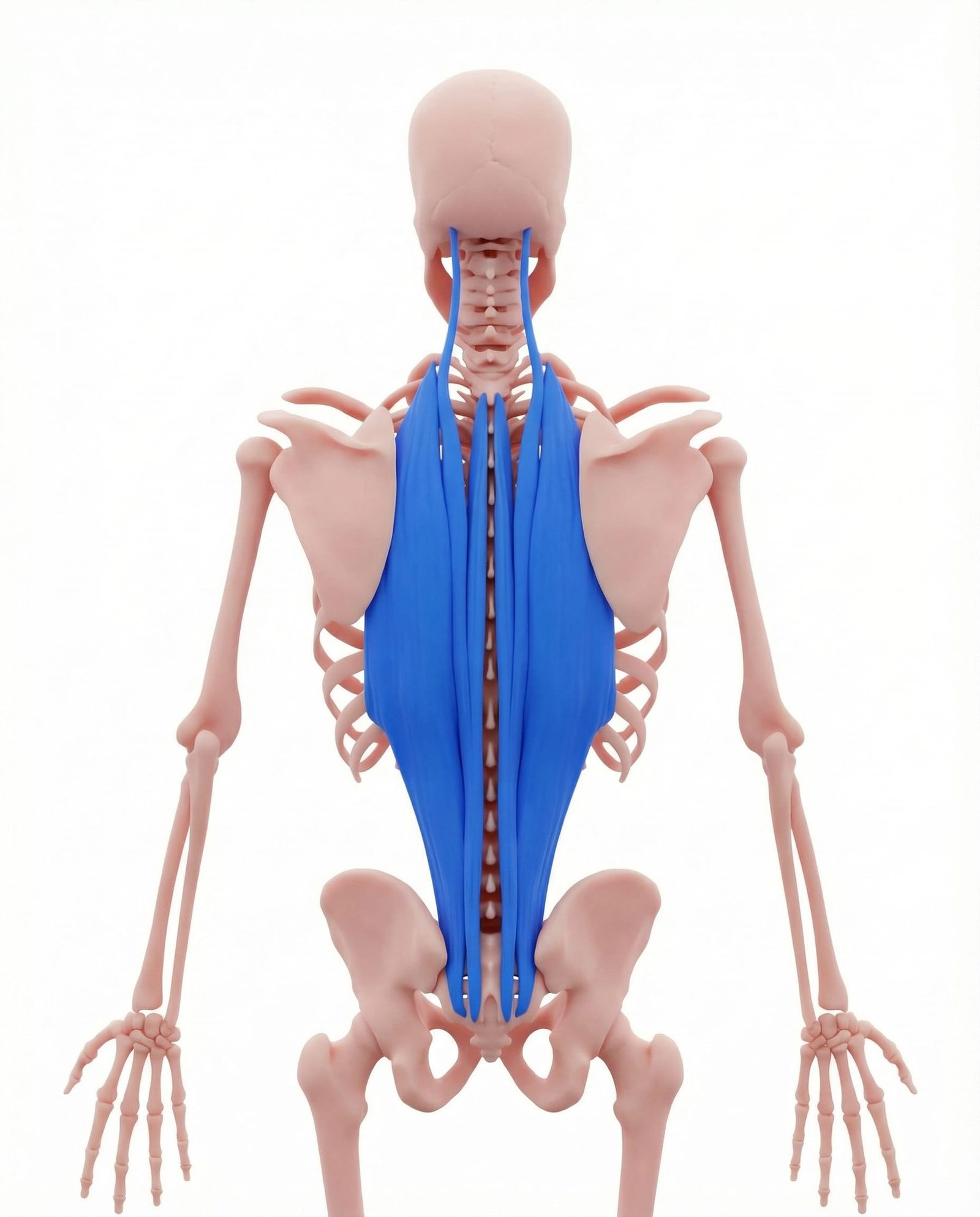
The hidden muscular causes behind the world's most common pain complaint — QL, multifidus, psoas, and more.
Cervical trigger points, text neck epidemic, and the headache connection — anatomy, self-tests, and treatment.
Rotator cuff and scapular trigger points that mimic tears, impingement, and frozen shoulder.
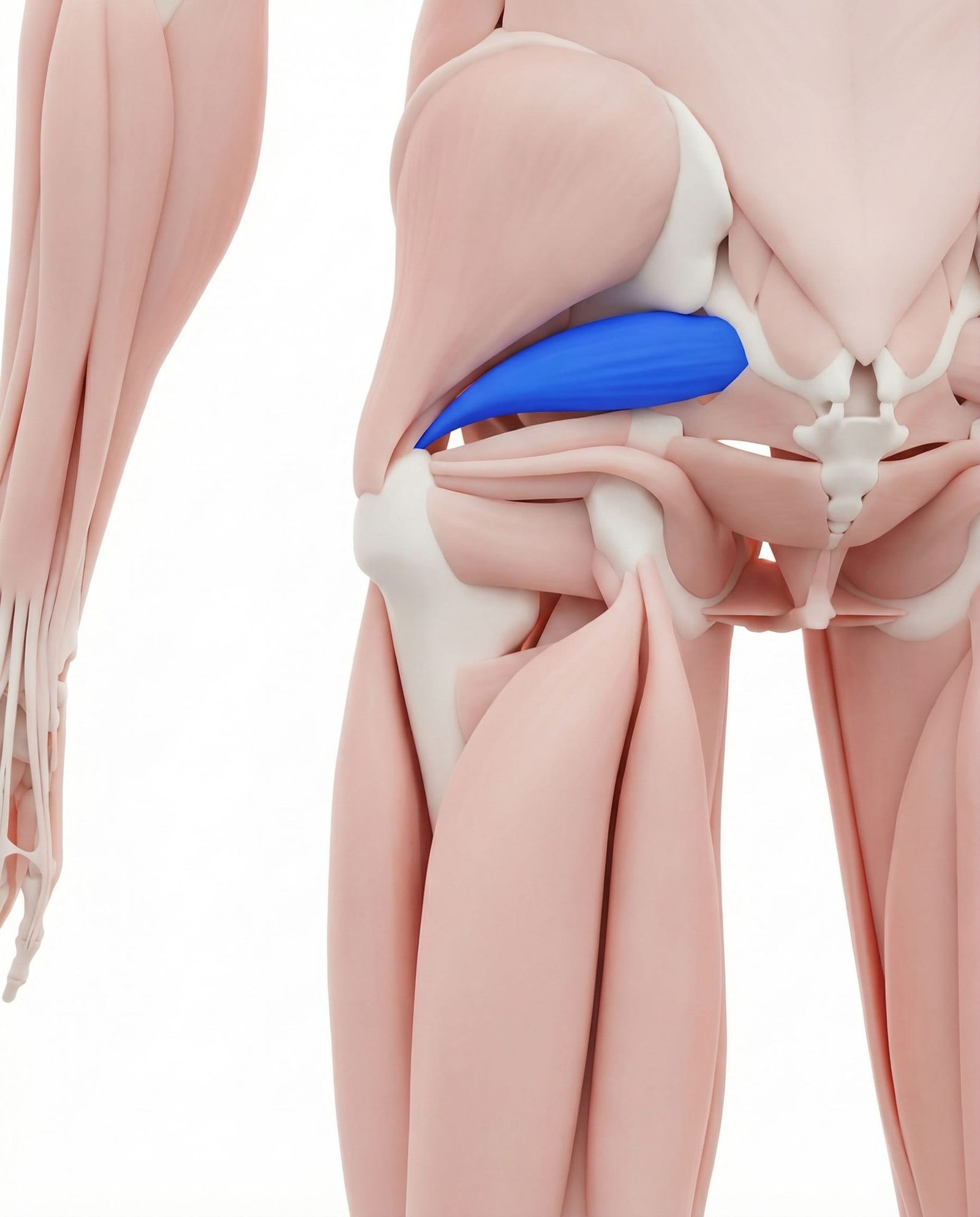
When a small deep hip muscle creates big sciatic-like pain — anatomy, FAIR test, and treatment pathways.
How jaw, face, and neck trigger points create temporomandibular dysfunction — bruxism, referral patterns, and relief.
Teeth grinding and clenching drive masseter, pterygoid, and temporalis trigger points — mimicking dental pain, ear pain, and chronic headache.
How pelvic floor, obturator internus, and lower abdominal trigger points mimic prostatitis, endometriosis, or chronic UTIs — and the specialized approach to treating them.
Why the gluteus medius and minimus are the true culprits behind most "hip bursitis" or "pseudo-sciatica" diagnoses — referral zones, sleep disruption, and targeted relief.
How trigger points in the vastus medialis, rectus femoris, and IT band refer deep, aching pain directly into the knee joint — mimicking meniscus tears and arthritis.
When stubborn bottom-of-foot pain isn't the fascia at all — how the gastrocnemius, soleus, and quadratus plantae refer pain straight to the heel.
How the supinator, brachioradialis, and wrist extensors create devastating elbow pain and grip weakness — saving patients from unnecessary steroid injections.
The "crush syndrome" effect: How scalene and pectoralis minor trigger points entrap nerves and refer aching pain, tingling, and numbness to the fingers.
The terrifying trigger points of the pectoralis major, sternalis, and intercostals that mimic heart attacks or rib dysfunction.
Untangling the confusion between regional trigger point pain and central sensitization — how they overlap, how to diagnose correctly, and why the treatment pathways differ.
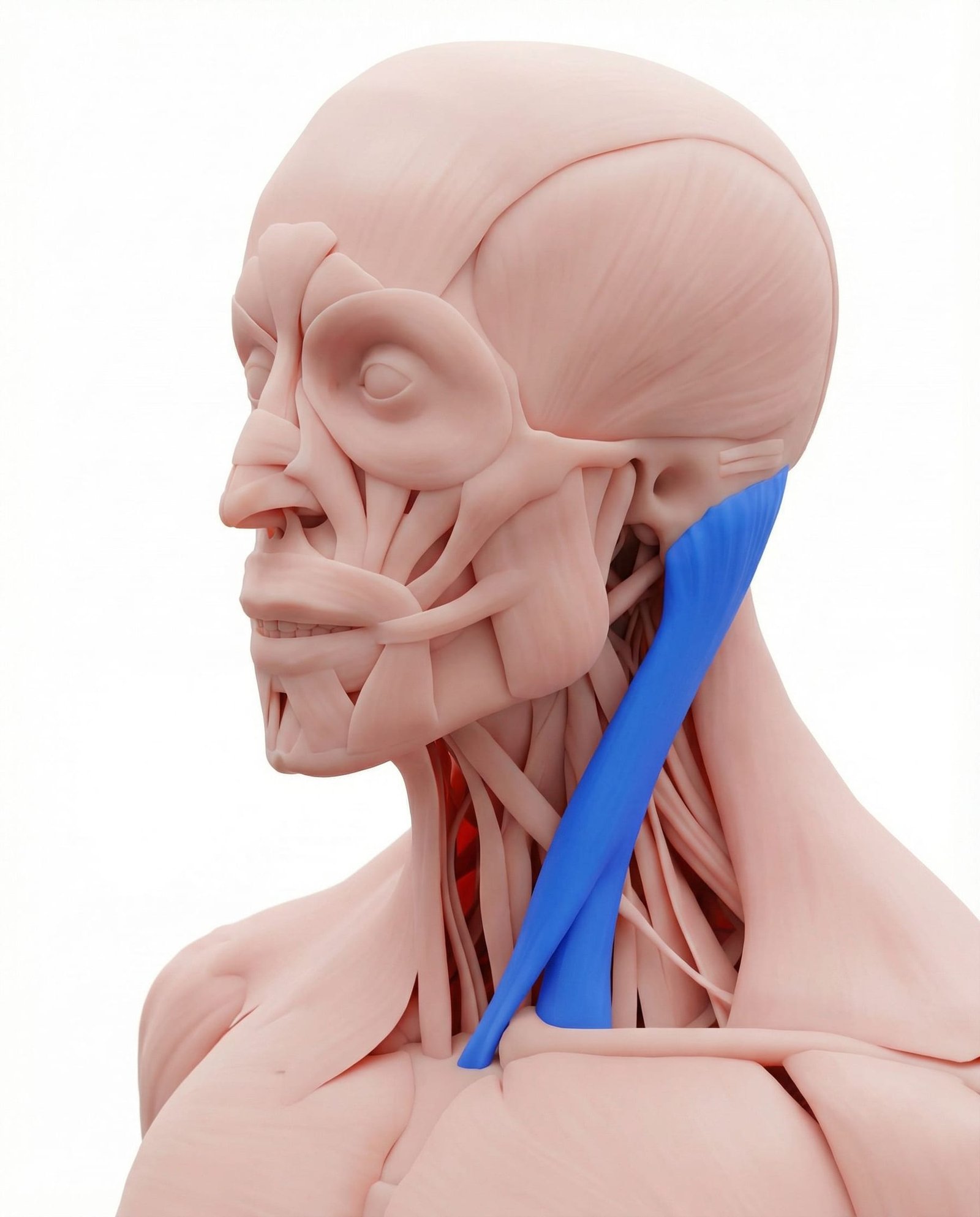
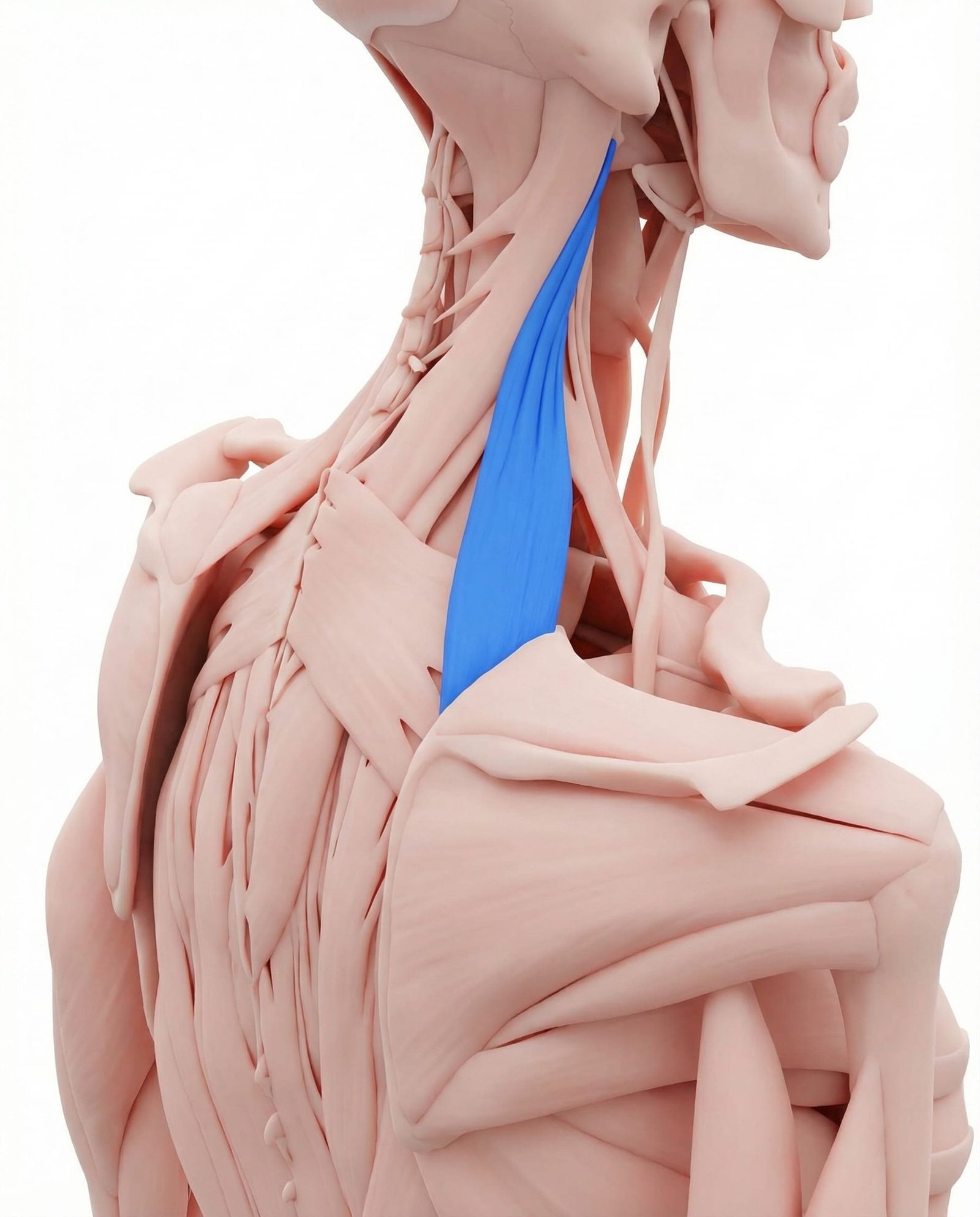
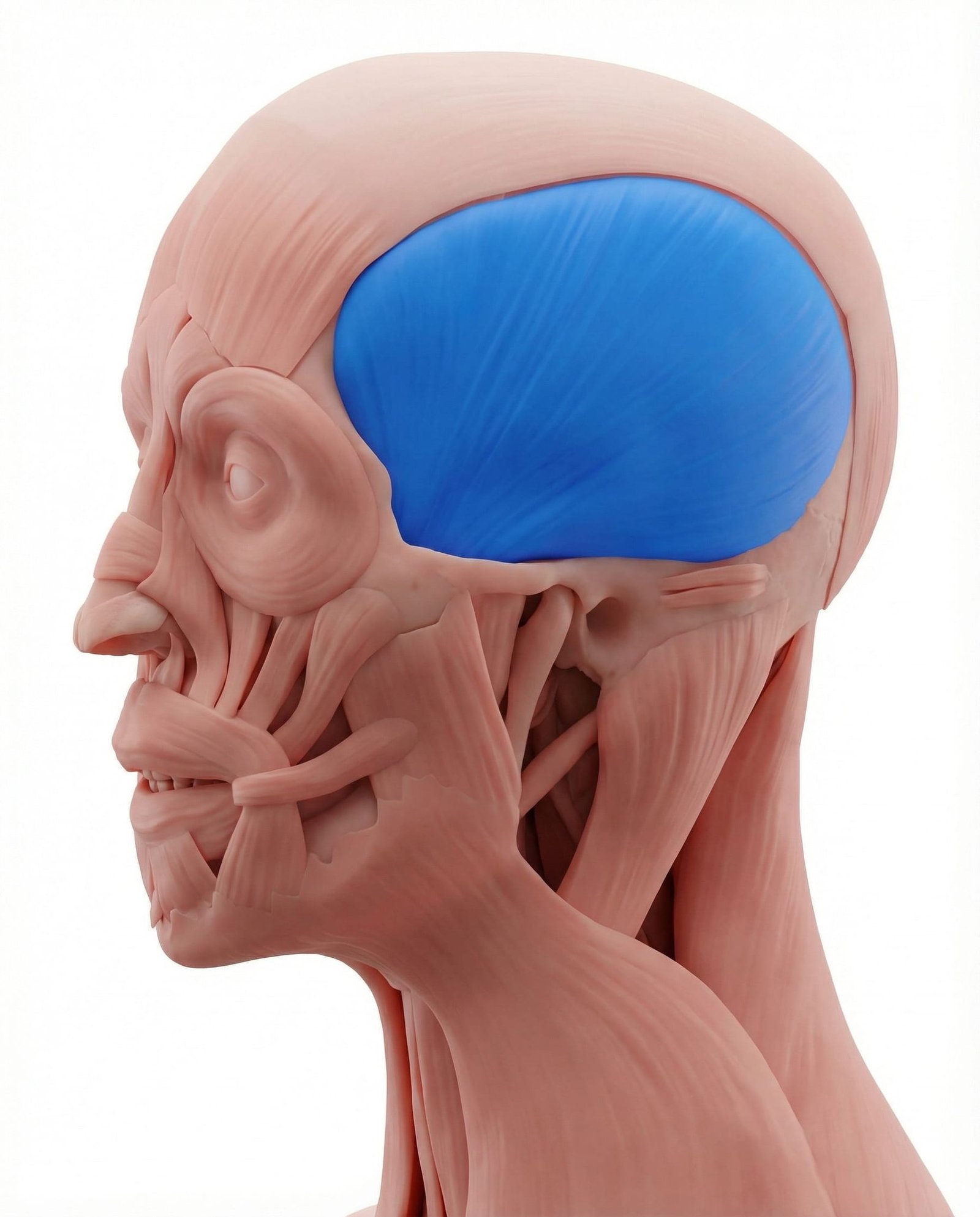
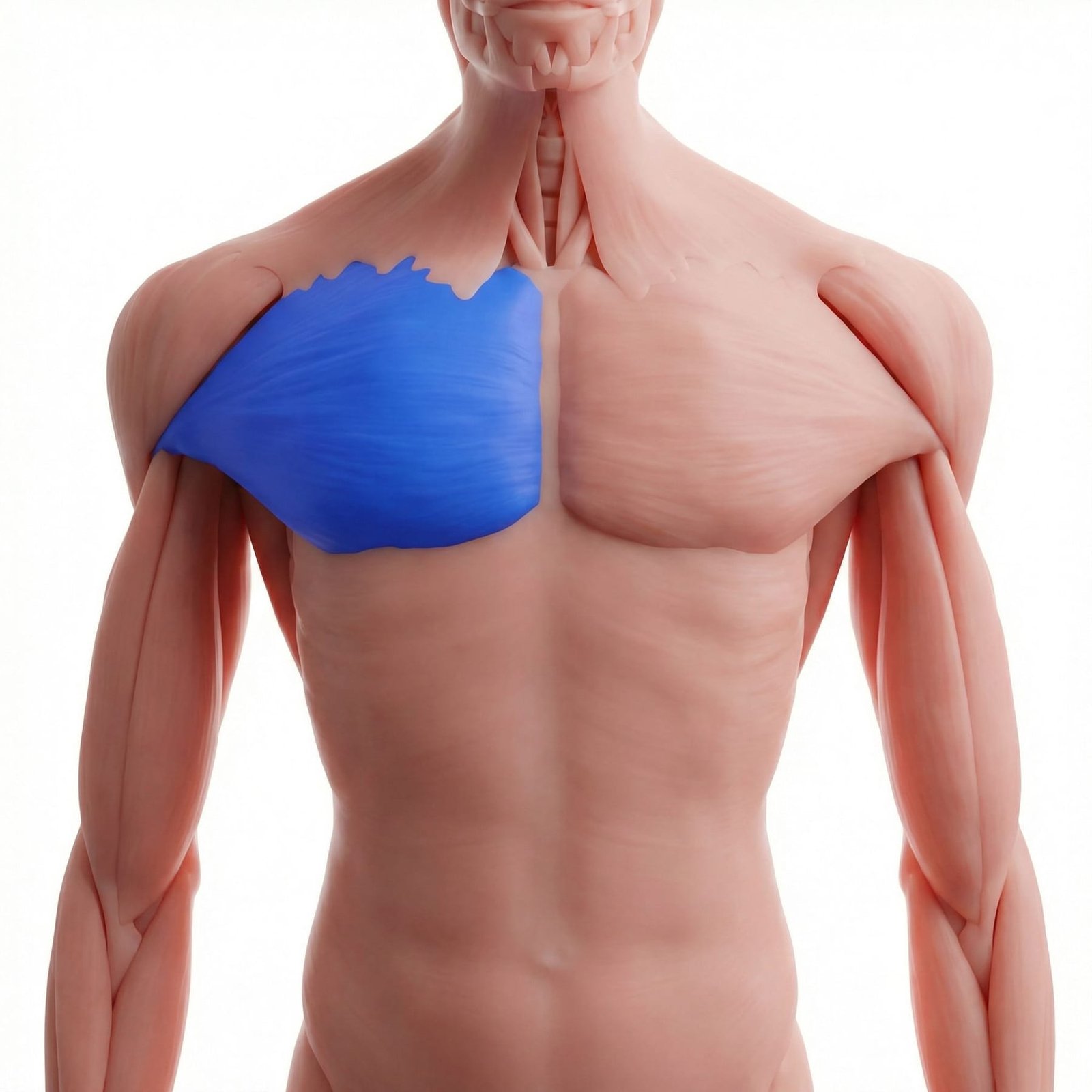
Muscle Deep Dives
Comprehensive anatomical guides for the muscles most commonly involved in chronic myofascial pain — trigger point maps, referral patterns, and treatment.









Understanding Trigger Points
Learn what trigger points are, how they are diagnosed, and why they are so often missed.
What is a trigger point? The anatomy, the energy crisis, taut bands, active vs. latent points, causes, and perpetuating factors.
Why myofascial pain takes 1-3 years to diagnose. The patient journey, common misdiagnoses, and how to find the right specialist.
A detailed comparison of two commonly confused conditions — differences in pain type, diagnosis, treatment, and prognosis.
The jump sign, local twitch response, satellite points, fake sciatica, phantom toothaches, and the wild history of trigger points.
Debunking common misconceptions about trigger points, myofascial pain, and chronic muscle conditions.
Flagged speculation: peripheral-central continuum, fascial revolution, AI-guided mapping, microbiome-pain axis, and psychoneuroimmunology.
Five phenotypes — local contracture, central sensitization, peripheral nerve, fascial, biomechanical — with matched treatments.
How a knot in your neck causes headaches, why your arm goes numb from a shoulder trigger point, and the jump sign.
The essential starting page for patients — what myofascial pain is, how it feels, how it differs from other conditions, and why there's good news.
What to expect during the diagnostic process — trigger point exams, tests that rule out other conditions, and emerging diagnostic tools.
How myofascial pain connects with fibromyalgia, migraine, TMJ, carpal tunnel, sciatica, IBS, and more — and why treating both matters.
How joint hypermobility contributes to chronic trigger points and what you can do about it.
The body's connective tissue web — fascial chains, how fascia creates and perpetuates trigger points, and why it matters for treatment.
When the nervous system turns up the volume on pain — how chronic pain rewires the brain, self-check tool, and treatment strategies.
Why your pain persists — understanding the transition from protective alarm to chronic disease, and how to break the cycle.
Direct, honest answers to 30+ questions patients ask most — from "Will this ever go away?" to "Is dry needling painful?"
How surgery creates trigger points, guarding patterns, and compensation chains — scar tissue mobilization, failed back surgery syndrome, and recovery.
How viral illness triggers widespread trigger points through inflammation, bed rest, and disrupted sleep — and how to recover without crashing.
Rumination, magnification, and helplessness — the three components of catastrophizing and why they predict pain outcomes more than imaging findings. Evidence-based interventions.
Kinesiophobia and pain-related fear explained — Vlaeyen's fear-avoidance cycle, the Tampa Scale, graded exposure therapy, and why telling patients to 'just push through it' is harmful.
A systematic clinical framework — distinguishing MPS from shoulder pathology, spinal conditions, headache disorders, and pelvic pain by region. Red flags, triage logic, and referral criteria.
Which symptoms are never myofascial — cauda equina, cancer-pattern pain, giant cell arteritis, cardiac referral. A clinical triage guide with urgency tiers and action steps.
MRI says 'disc bulge' — does it explain your pain? Understanding incidental findings, nocebo effect of radiological reports, and why normal-looking scans don't mean normal function.
Complex Regional Pain Syndrome versus Myofascial Pain Syndrome — overlapping symptoms, Budapest Criteria, sympathetic nervous system involvement, and when to suspect CRPS.
The gut-brain-muscle axis — how irritable bowel syndrome and abdominal MPS are linked through shared sensitization pathways, viscero-somatic reflexes, and Carnett's sign.
How obstructive sleep apnea and myofascial pain fuel each other — intermittent hypoxia, pro-inflammatory cytokines, jaw bruxism, and cervical trigger points. Breaking the vicious cycle.
Shared neurobiology — HPA axis dysregulation, limbic pain amplification, and descending inhibition. Why SNRIs help MPS pain even without depression, and the evidence for integrated treatment.
Medications & Pharmacology
Complete pharmacology guides — from OTC analgesics to interventional pharmacotherapy. Mechanism of action, dosing, evidence, and practical prescribing.
Complete overview of OTC, prescription, adjuvant, and injection therapies. Pharmacological hierarchy and why opioids fail.
Evidence-based supplements — magnesium, vitamin D, CoQ10, omega-3s — anti-inflammatory diets, and nutritional strategies for myofascial pain.
Common mistakes patients and practitioners make that worsen trigger points or prevent recovery.
Ibuprofen, naproxen, diclofenac, celecoxib — COX inhibition, topical vs oral, GI/CV/renal risks, and practical prescribing for myofascial pain.
Acetaminophen and Dipyrone (Metamizole). Mechanisms, dosing, hepatotoxicity, agranulocytosis debate, and combination products.
Cyclobenzaprine, tizanidine, methocarbamol, orphenadrine, baclofen. Central mechanisms, individual profiles, and short-term use guidelines.
TRPV1 receptor desensitization, substance P depletion, OTC creams vs Qutenza 8% patch, and how to use effectively for trigger points.
Lidoderm 5% patch, creams, EMLA. Sodium channel blockade, clinical evidence, and application guide for myofascial trigger points.
Amitriptyline, nortriptyline, desipramine. Dual neurotransmitter reuptake, sodium channel blockade, NMDA antagonism — gold standard adjuvant.
Duloxetine, venlafaxine, milnacipran. FDA-approved for chronic pain. Central sensitization targeting and descending inhibition enhancement.
Gabapentin and pregabalin. Alpha-2-delta calcium channel ligands. Wind-up reduction, central sensitization, and when to use for myofascial pain.
Why opioids are ineffective and harmful for myofascial pain. Wrong mechanism, hyperalgesia, guideline recommendations, and better alternatives.
Non-psychoactive cannabinoid acting via FAAH inhibition, TRPV1 agonism, adenosine reuptake, and anti-inflammatory pathways. Topical, sublingual, and oral formulations.
The most injected anti-inflammatory class. Triamcinolone, dexamethasone, methylprednisolone — PLA2 inhibition, NF-κB suppression, and use-limited protocols.
Off-label opioid antagonist paradox: TLR4 antagonism, microglial M1→M2 shift, endogenous opioid rebound. Unique mechanism at 1-4.5mg dosing.
B1, B6, B12 mechanisms for nerve repair and pain modulation — complete clinical guide.
Custom transdermal medications — ketoprofen, baclofen, gabapentin, cyclobenzaprine in PLO gel. High-concentration local delivery with minimal systemic side effects.
Practical comparison guide — why tizanidine is preferred for MPS, cyclobenzaprine's 18h half-life problem, and why carisoprodol should be avoided.
Beyond CBD — THC:CBD ratios, endocannabinoid system, routes of administration, opioid-sparing evidence, and practical clinical guide.
Chlorpromazine (Amplictil), levomepromazine (Neozine), quetiapine — D2 blockade for treatment-resistant pain, sedation as a tool, and cautious off-label use in refractory cases.
GABA-A agonists that mask symptoms without treating trigger points. High dependence risk, impaired motor learning, and why safer alternatives exist.
Trazodone, Z-drugs (zolpidem, eszopiclone), and suvorexant — restoring Stage 3/4 NREM sleep as a treatment strategy for chronic MPS.
Clonidine, tizanidine, and dexmedetomidine — central sympatholytic agents that reduce sympathetic hyperactivity maintaining trigger points.
Glycinate, malate, and threonate forms — physiological muscle relaxant, NMDA antagonist, and calcium regulator. 50-80% of population deficient.
Interventional & Device Therapies
Needle-based, device-based, and hands-on clinical treatments — from dry needling to neuromodulation.
Sortable, filterable comparison of HILT (iLux Smart, Hiro, K-Laser, LightForce) and LLLT platforms (THOR, MR4, BioFlex, Erchonia) — power, wavelength, penetration, dose, and RCT outcomes for musculoskeletal pain.
How filiform needles target trigger points to elicit local twitch responses. Techniques, mechanisms, evidence, and what to expect.
Traditional and Western medical acupuncture for myofascial pain. Mechanisms, point selection, evidence from clinical trials.
Lidocaine, procaine, and saline injections directly into trigger points. Protocols, comparisons, and clinical outcomes.
Botulinum toxin for chronic, refractory myofascial pain. Mechanism, dosing, evidence, ideal candidates, and cost considerations.
Focused and radial extracorporeal shockwave therapy for trigger points. Non-invasive, 78-85% success rate, and growing evidence base.
Percutaneous electrical nerve stimulation — needle electrodes delivering current past skin impedance for 10-100× more efficient stimulation than TENS.
Electrical stimulation through acupuncture needles. Frequency-dependent opioid release, standardized dosing, and enhanced analgesia for myofascial pain.
Autologous platelet-rich plasma injections for trigger points. Growth factors, tissue regeneration, and emerging evidence for refractory myofascial pain.
French intradermal microinjection technique. Multi-agent cocktails (procaine, piroxicam, B12) targeting pain at the source — peu, rarement, au bon endroit.
Regenerative injection therapy with hypertonic dextrose. Controlled inflammation triggers collagen synthesis, fibroblast proliferation, and tissue repair.
Ultrasound-guided tissue plane separation for fascial adhesions and nerve entrapment — cluneal, dorsal scapular, spinal accessory nerve liberation.
Myofascial decompression through negative pressure — wet, dry, and sliding cupping for trigger point release.
NMDA receptor blockade and central sensitization reversal — sub-anesthetic IV, intranasal, and oral ketamine protocols for treatment-resistant myofascial pain.
Graston, HawkGrips, and FAKTR protocols — fibroblast activation science, region-specific applications, and a comparison with manual soft tissue therapy.
Chan Gunn's neuropathic model for treating chronic myofascial pain through deep intramuscular needle stimulation — with comparison to dry needling approaches.
Prolotherapy, platelet-rich plasma (PRP), and stem cell therapies compared — current evidence, appropriate patient selection, cost realities, and the future of regenerative medicine for MPS.
Class IV Nd:YAG laser (1064nm, 6-12W) for deep tissue trigger point deactivation. Photobiomodulation, thermal gradients, and 60-80% pain reduction in 4-6 sessions.
Ultrasound-guided regional anesthesia targeting fascial compartments — ESP blocks, Pecs I/II, serratus anterior plane, and QL blocks for refractory myofascial pain.
Targeted neural blockade for diagnostic and therapeutic management — greater occipital, suprascapular, intercostal, and sciatic blocks when MPS coexists with nerve entrapment.
Capacitive and resistive electric transfer (448 kHz) for endogenous deep tissue heating. Reaches 3-4 cm depth with 4-7°C temperature increase for trigger point deactivation.
Systemic sodium channel blockade for widespread, centrally sensitized myofascial pain. 1-5 mg/kg/hr over 1-4 hours with cardiac monitoring — 40-60% pain reduction.
18 evidence-based physical therapies: acupuncture, dry needling, shockwave, laser, cupping, TENS, fascial manipulation, and more.
Ischemic compression, myofascial release, deep tissue, spray-and-stretch, strain-counterstrain, and muscle energy techniques.
Transcutaneous electrical nerve stimulation for self-administered pain relief. Modes, electrode placement, home use guide.
Autonomic neuromodulation via the vagus nerve. Anti-inflammatory reflex, tVNS devices, and practical self-stimulation techniques.
Transcranial direct current stimulation and transcranial magnetic stimulation — brain-level neuromodulation for central sensitization.
Understanding how pain works in the nervous system. Grade A evidence for reducing catastrophizing, fear-avoidance, and disability.
Active and passive treatments — manual release, dry needling, ultrasound, therapeutic exercise, neuromuscular re-education, and progressive loading protocols.
The 3-phase protocol: Deactivate Pain → Restore Function → Prevent Recurrence. A structured, evidence-based pathway for full myofascial pain recovery.
Where most clinicians miss: mixed pain states, phenotype-based treatment, the needle effect, fascial under-treatment, and premium clinic protocols.
Interactive quiz: answer 6 questions about your situation and get personalised treatment recommendations ranked by evidence and cost.
Which practitioners do what, how to evaluate if they understand myofascial pain, questions to ask, red flags, and sample care team configurations.
Self-Care & Movement
Everything you can do at home — from foam rolling and stretching to yoga, Tai Chi, and aquatic therapy. Practical daily management.
Self-massage techniques, foam rolling, heat/cold therapy, stretching, ergonomics, sleep hygiene, and lifestyle modifications.
Interactive guided questionnaire: Does your pain travel? Does pressing reproduce it? Get your likely muscle source and learn when to seek professional care.
Select your trigger point and get a customized home plan — specific stretches, strengthening exercises, self-release techniques, and heat vs cold guidance per muscle.
Workstation setup, driving ergonomics, phone use, sleep positions, and movement breaks — specific to trigger point prevention.
Step-by-step protocol for the first 24, 48, and 72 hours of a pain flare-up — what to do, what NOT to do, and when to call for help.
How stress physically creates trigger points — the autonomic loop, where your body holds stress, and practical techniques to break the cycle.
Foods that fight inflammation, nutrients for muscle health, the gut-pain axis, anti-inflammatory plate builder, and sample meal plans.
Complete guide to foam rollers, massage balls, massage guns, and hook tools — choosing the right tool, techniques by body region, and common mistakes.
Red flags vs. typical myofascial pain symptoms — know the difference between what's normal and what needs urgent medical attention.
How to describe your symptoms clearly, ask the right questions, advocate for trigger point assessment, and handle dismissal.
From ancient Chinese "Ah Shi" points to Travell & Simons, JFK's physician, and modern elastography imaging.
Beyond generic sleep hygiene — pillow height formulas by pain location, cervical roll specifications, body pillow configurations, and position strategies for common MPS presentations.
Seat, headrest, and pedal configuration for lumbar, gluteal, and cervical MPS — long-drive break strategies and how vehicle setup manages whiplash-associated trigger point perpetuation.
Learn to locate your own trigger points — taut band identification, pressure algometry concepts, referred pain mapping, and safe self-palpation techniques by body region.
Master the tools and techniques — foam rollers, massage balls, and hands-on self-treatment. Body-region techniques, pressure guidelines, and daily protocols.
Evidence-based guide to Theragun and massage guns — settings, attachment heads, technique by body region, and when to use vs. foam rolling.
Static vs. dynamic, PNF, active isolated — when each is appropriate, the correct sequence, and safety principles for myofascial pain.
The ultimate guide to temperature therapy for MPS — why heat melts trigger points, when ice makes spasms worse, contrast therapy protocols, and safe application times.
Transcutaneous Electrical Nerve Stimulation for home use — pad placement maps for common trigger points, optimal frequency settings, and safety limits.
How to use Shakti mats, TheraCanes, and Backnobbers — ischemic compression, gate control theory at home, and targeting hard-to-reach trigger points.
The #1 hidden perpetuator of chronic myofascial pain — cervical pillow selection, knee bolsters for pelvic torsion, mattress firmness, and sleep posture correction.
Combating Upper Crossed Syndrome and tech neck — monitor height, chair lumbar support, desk setup, and the 20-minute micro-break protocol.
Core stability, controlled movement, and flexibility — integration with release work, 8 key exercises, props guide, and beginner protocol.
Ancient meditative movement meets modern pain science — 8 key movements, evidence base, and getting started guide.
Clinically recommended for persistent trigger points — 10 poses, 5 yoga styles compared, safety guidelines, and 4-week beginner program.
Progressive resistance programs — 4-phase protocol, exercises by body region, training principles for pain patients, and sample weekly programs.
Safe exercises for myofascial pain patients — the 3-phase approach, best activities, stretching techniques, and a daily movement minimum.
Dysfunctional breathing creates 17,000 scalene contractions daily — the critically overlooked perpetuating factor in cervical and shoulder MPS.
90% success at 12 weeks — why slow lengthening contractions heal where concentric exercise irritates. Achilles, rotator cuff, patellar, and hamstring protocols.
Nerve flossing and sliding for MPS with nerve involvement — median, ulnar, radial, and sciatic nerve protocols integrated with trigger point treatment.
Restoring joint position sense breaks the perpetuating cycle — cervical laser exercises, single-leg progressions, and multifidus reactivation protocols.
Diaphragmatic re-education, capnometry biofeedback, and clinical breathing rehabilitation — structured protocols for cervical and thoracic trigger point management.
Mechanical Diagnosis and Therapy — directional preference assessment, centralization phenomenon, and patient-led spinal exercise protocols for myofascial and discogenic pain.
EDS, BJHS, and generalized joint hypermobility — specific stabilization protocols that strengthen without destabilizing. Beighton score, co-contraction training, and progressive loading.
Buoyancy reduces joint load while water provides natural resistance — exercises by condition, swimming strokes, and AquaStretch™ techniques.
Simpler than Tai Chi, profoundly calming — 8 key movements, seated modifications, and a 4-week beginner protocol for stress-related trigger points.
Not just "go for a walk" — proper form, pacing strategies, the boom-bust cycle, and walking programs by pain stage.
Long-held, prop-supported poses for deep fascial release and nervous system regulation — 16 poses, props guide, and sample sequences.
Halliwick, Watsu, and Bad Ragaz Ring Method — three specialized aquatic approaches that go far beyond basic pool exercises for complex chronic myofascial pain.
Props, precision, and alignment — using bolsters, blocks, straps, and wall support to make therapeutic yoga accessible and safe for myofascial pain, hypermobility, and restricted mobility.
Cognitive behavioral strategies for chronic pain — restructuring thoughts, graded exposure, relaxation training, and acceptance.
The #1 perpetuating factor for myofascial pain. Sleep hygiene, positions, CBT-I, medications for sleep, and the pain-sleep vicious cycle.
Train your brain to change its relationship with pain — MBSR, body scan techniques, guided exercises, and the fMRI evidence behind it.
KT Tape, RockTape, and Kinesio techniques — specific application patterns for trapezius, lumbar, and patellar MPS, with honest appraisal of what the evidence supports.
When supports help and when they harm — cervical collars, lumbar belts, wrist splints, proper wear schedules, and a structured protocol for weaning off bracing.
Special Populations
Tailored guidance for caregivers, older adults, men, women, and athletes — because one size doesn't fit all.
Research Library
Plain-language summaries of 100+ peer-reviewed studies on myofascial pain — with visual data, key findings, and patient takeaways.