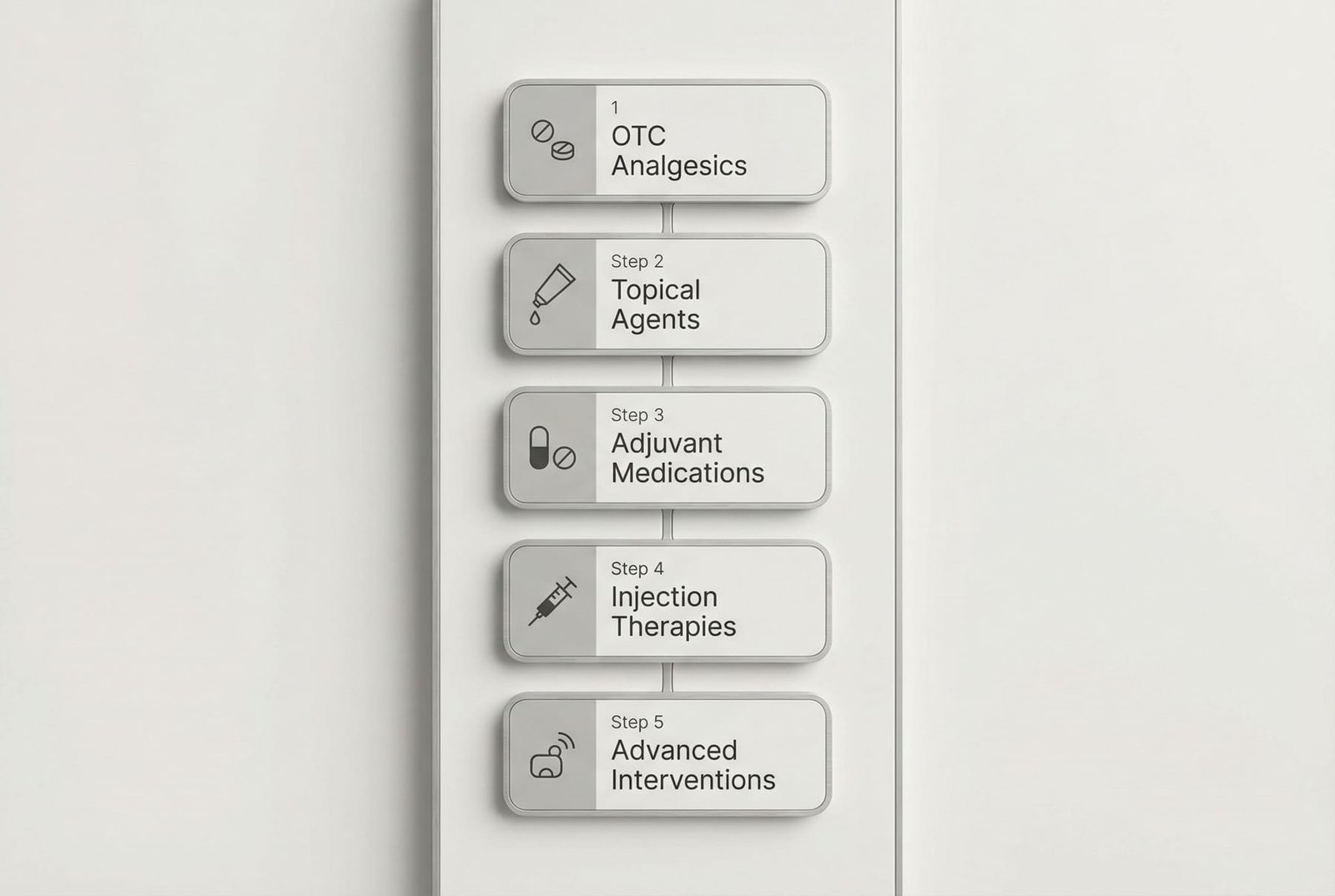
Pharmacological Approach Hierarchy
Medication management for myofascial pain is usually stepwise and individualized. The aim is to use the least burdensome option that meaningfully helps, while still prioritizing rehabilitation and self-management.
No single medication treats all aspects of myofascial pain. The best results usually come from combining appropriate pharmacology with physical care and active recovery.
Medications
Mechanism of Action DiagramOTC Analgesics
Start with the simplest lower-risk options when appropriate. Not every patient needs to move beyond this step.
Topical Agents
Targeted local treatment may be added when the painful region is superficial and accessible.
Adjuvant Medications
When pain becomes broader, more chronic, more sleep-disruptive, or more centrally amplified, adjuvant medications may be considered by a clinician.
Injection Therapies
Focal procedures may be considered in selected patients with persistent, clearly identified trigger-point or inflammatory overlap problems.
Advanced Interventions
Reserved for refractory cases under specialist care and usually only as part of a broader multimodal plan.
Over-the-Counter (OTC) Analgesics
These are often the starting point for mild to moderate symptoms, but they do not replace rehabilitation or address every driver of trigger point pain.
Acetaminophen (Tylenol / Paracetamol)
Localized or mild pain when anti-inflammatory effect is not the main goal
Mechanism of Action
Primarily a centrally acting analgesic. It may help reduce pain intensity, but it is not generally viewed as a strong anti-inflammatory option for myofascial pain.
Typical Dosing
Use only according to product labeling or clinician guidance
Advantages
- No direct NSAID-type stomach irritation
- Can be used as a simpler first-line analgesic in some situations
- May fit patients who cannot take NSAIDs
Disadvantages
- Often limited for more persistent myofascial pain
- Does not address inflammation directly
- Liver safety still matters, especially with alcohol use or liver disease
NSAIDs (Ibuprofen, Naproxen, Diclofenac)
Pain relief when inflammation or flare-related irritation seems relevant
Mechanism of Action
NSAIDs reduce prostaglandin-mediated pain signaling and may help when pain has an inflammatory or post-treatment soreness component.
Typical Dosing
Use only according to product labeling or clinician guidance
Advantages
- Common and widely available
- Often more helpful than acetaminophen when inflammation is part of the pain picture
- Topical diclofenac offers a lower-systemic-exposure option
Disadvantages
- GI, kidney, and cardiovascular risks still matter
- Not ideal as chronic default treatment without review
- May not meaningfully change the underlying drivers of trigger points
Dipyrone (Metamizole / Dipirona)
Acute musculoskeletal or spasm-related pain in regions where it is available and medically accepted
Mechanism of Action
A centrally acting analgesic with spasmolytic properties that is commonly used in some countries for acute pain states.
Typical Dosing
Use only according to local product labeling and clinician guidance
Advantages
- Can be a useful non-opioid analgesic in regions where it is familiar
- Often considered when NSAIDs are poorly tolerated
- Has a long history of use in some countries
Disadvantages
- Not available in many countries
- Hematologic safety concerns remain important
- Should not be treated as universally interchangeable with other OTC analgesics
Prescription Pain Medications
Prescription analgesics are usually considered only when pain severity, chronicity, or associated central sensitization makes simpler options insufficient.
Tramadol (Ultram)
Selected moderate to severe pain when simpler options are inadequate and a clinician believes the risk-benefit balance is acceptable
Mechanism of Action
A centrally acting analgesic with both weak opioid activity and monoamine reuptake effects. It is sometimes used for more severe pain, but it is not a first-line solution for ordinary myofascial pain.
Typical Dosing
Specialist or clinician-directed only
Advantages
- Can provide stronger analgesia than simple OTC options
- Has mixed analgesic mechanisms
- May be considered when other strategies have failed
Disadvantages
- Still carries dependence, sedation, seizure, and serotonin-syndrome concerns
- Not appropriate as routine long-term myofascial treatment
- Can complicate rehabilitation by increasing sedation or cognitive burden
Muscle Relaxants (Cyclobenzaprine, Tizanidine, Methocarbamol)
Short-term symptom management when muscle spasm, guarding, or sleep disruption is prominent
Mechanism of Action
These agents reduce muscle-related discomfort through centrally acting sedative or motor-modulating effects rather than by directly “deactivating” a trigger point.
Typical Dosing
Specialist or clinician-directed only
Advantages
- May help break a short-term spasm-pain cycle
- Can be useful when sleep is being disrupted by muscular pain
- Sometimes helpful as a bridge while rehabilitation is getting started
Disadvantages
- Sedation and cognitive slowing are common limitations
- Not ideal for indefinite use
- Do not replace strengthening, movement retraining, or load correction
Adjuvant Medications
These medications are often most relevant when myofascial pain overlaps with sleep problems, anxiety, neuropathic symptoms, or broader pain amplification.
Tricyclic Antidepressants (Amitriptyline, Nortriptyline)
Class: Antidepressant (TCA)
Mechanism of Action
These medications are used in pain care because they can affect descending pain-modulating pathways and sleep quality. Their pain role is distinct from their use in depression.
Typical Dosing
Clinician-directed only
Benefits
- Can help sleep as well as pain in selected patients
- Long history of use in chronic pain medicine
- Useful when pain is not purely mechanical and local
Considerations
- Side effects and overdose safety matter
- Not everyone tolerates anticholinergic burden well
- Need gradual adjustment and follow-up
SNRIs (Duloxetine, Venlafaxine, Milnacipran)
Class: Antidepressant (SNRI)
Mechanism of Action
These medications are used in chronic pain because they can enhance descending inhibitory pain pathways and may also help mood and anxiety symptoms when those overlap with pain.
Typical Dosing
Clinician-directed only
Benefits
- Relevant when pain and mood symptoms overlap
- Can fit more widespread pain states better than purely local treatments
- Often better tolerated than TCAs in some patients
Considerations
- Nausea, blood pressure effects, and discontinuation symptoms matter
- Do not work immediately
- Need monitoring and gradual changes
Gabapentinoids (Gabapentin, Pregabalin)
Class: Anticonvulsant / Neuromodulator
Mechanism of Action
These medications are used when central sensitization, neuropathic-like symptoms, allodynia, sleep disruption, or broader pain amplification seem clinically relevant.
Typical Dosing
Clinician-directed only
Benefits
- May help more when pain is amplified or neuropathic-like
- Can support sleep in some patients
- Useful in selected broader pain phenotypes
Considerations
- Sedation, dizziness, edema, and misuse concerns matter
- Need slow titration and tapering
- Not ideal for every myofascial pain patient
Topical Agents (Diclofenac Gel, Lidocaine Patches, Capsaicin)
Class: Topical analgesic / Local anesthetic
Mechanism of Action
Topical treatments aim to provide local symptom relief with less systemic exposure than oral medication. Their usefulness depends heavily on whether the painful region is superficial and well localized.
Typical Dosing
Use according to product labeling or clinician guidance
Benefits
- Targeted application
- Lower systemic exposure than many oral agents
- May fit patients trying to avoid more sedating or systemic options
Considerations
- Skin irritation is common enough to matter
- Depth is limited
- Different products have different rules and risks
Emerging & Complementary Options
These treatments are discussed increasingly in chronic pain care, but evidence, regulation, and product quality vary widely.
CBD (Cannabidiol)
Adjunctive use in selected chronic pain patients under appropriate medical and legal guidance
Mechanism of Action
CBD is often discussed in chronic pain because of possible effects on stress, sleep, inflammation, and pain modulation. It should be presented cautiously, since product quality and evidence are highly variable.
Dosing & Bioavailability
Do not self-direct; use only according to product labeling or clinician guidance
Potential Benefits
- Often perceived as more tolerable than THC-containing products
- May be relevant when sleep or anxiety overlaps with pain
- Can be used topically or systemically depending on product type
Limitations & Risks
- Product quality is inconsistent
- Drug interactions matter
- Myofascial pain-specific evidence is limited
- Legal and regulatory issues vary widely
Injection Therapies
Procedural treatments may be useful when a focal pain generator is clearly identified or when conservative care has not been enough.
Local Anesthetic Trigger Point Injections (TPI)
Best for: Selected focal trigger points that have not responded to simpler careA clinician-directed focal injection used in selected patients when a specific trigger point has remained active despite simpler treatment. It is best viewed as a targeted procedural option rather than routine care for all MPS.
Mechanism
Local anesthetic effect plus mechanical disruption of a focal trigger point region
Dosing & Protocol
Procedure-specific and clinician-directed only
Key Benefits
- May provide quick local pain relief
- Can help confirm whether a focal trigger point is clinically relevant
- May create a window for stretching or rehab afterward
Corticosteroid Injections
Best for: Inflammatory overlap rather than simple isolated trigger pointsSometimes considered when a trigger-point-like presentation overlaps with a more clearly inflammatory local condition such as bursitis or tendinopathy. They should not be portrayed as routine trigger point care.
Mechanism
Local anti-inflammatory effect
Dosing & Protocol
Procedure-specific and clinician-directed only
Key Benefits
- May help when inflammation is truly part of the problem
- Can provide longer symptom relief in selected inflammatory cases
Botulinum Toxin Type A (BOTOX, Dysport, Xeomin)
Best for: Selected refractory casesA specialist intervention sometimes discussed in chronic refractory myofascial pain, especially when repeated simpler treatments have failed. It should not be presented as routine early care.
Mechanism
Neuromuscular blockade with possible secondary pain-modulating effects
Dosing & Protocol
Procedure-specific and clinician-directed only
Key Benefits
- Longer-lasting than many local procedures in selected cases
- May help when muscle overactivity is a major driver
Prolotherapy (Regenerative Injection Therapy)
Best for: Selected chronic cases with instability or connective tissue contributionSometimes discussed when trigger points coexist with ligament laxity, joint instability, or tendon-related overload. It belongs more to selected regenerative-medicine conversations than to routine MPS care.
Mechanism
Localized proliferative / regenerative response model
Dosing & Protocol
Procedure-specific and clinician-directed only
Key Benefits
- May be relevant when instability is part of the perpetuating problem
- Sometimes considered in more chronic mixed structural-myofascial cases
Mesotherapy (Intradermal Microinjections)
Best for: Selected localized pain care in practices where the method is establishedA superficial microinjection technique used in some countries and practices for localized pain. Because formulations and standards vary widely, it should be described cautiously and regionally rather than as a universal evidence-based default.
Mechanism
Localized superficial pharmacologic and sensory-stimulation effects
Dosing & Protocol
Procedure-specific and clinician-directed only
Key Benefits
- Localized treatment with lower systemic exposure in some protocols
- Often discussed for regionally limited pain
Why Opioids Are Usually a Poor Fit
Opioids generally fit poorly with a condition that requires movement recovery, self-management, and treatment of perpetuating factors rather than escalating sedation.
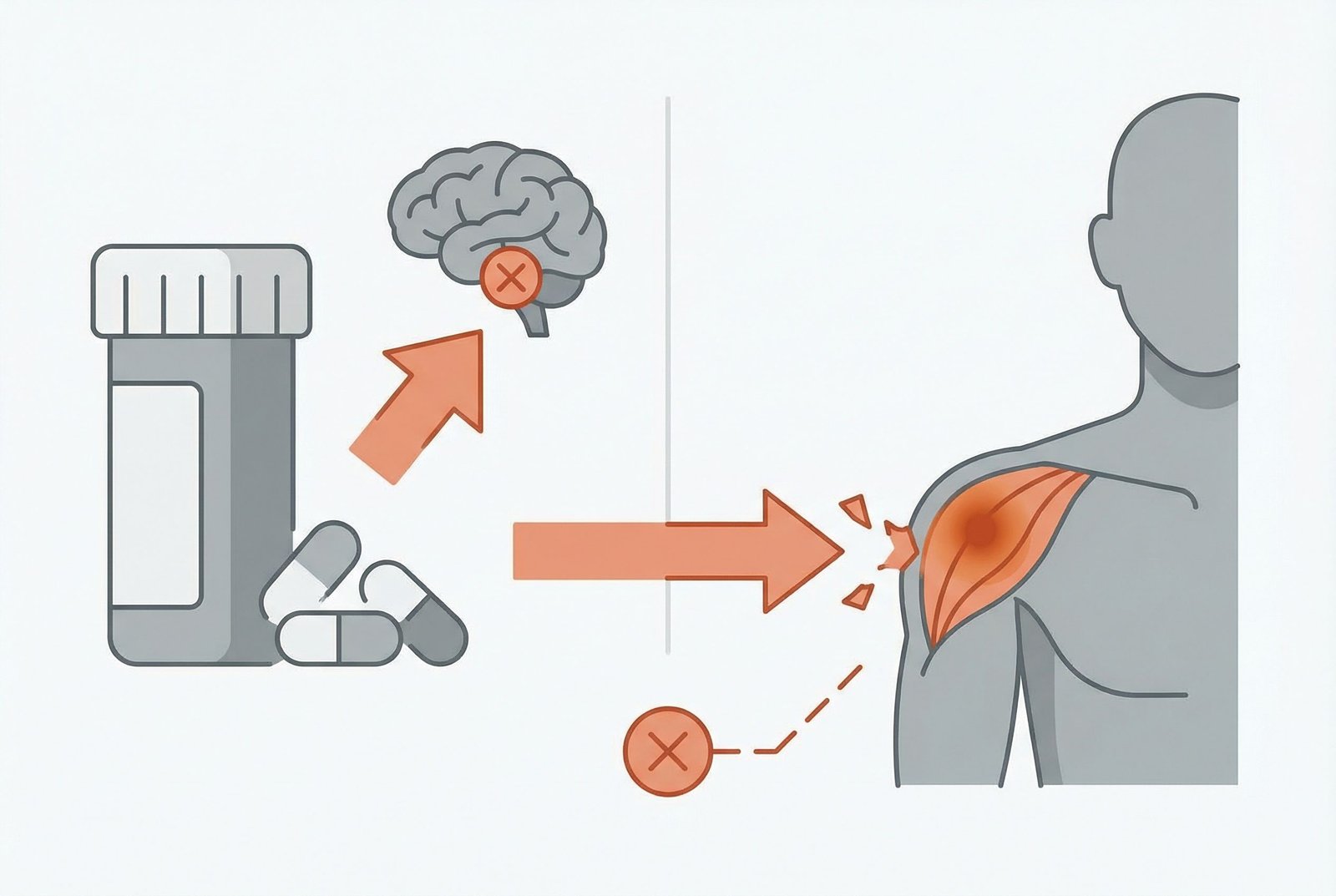
Why Opioids Are Ineffective for Myofascial Pain
Mechanism DiagramBottom line: Most modern pain guidelines do not position opioids as a routine treatment for myofascial pain. A multimodal approach — physical therapy, clinician-directed trigger point work, non-opioid pharmacotherapy, and self-management — is generally considered both safer and more effective.
They Do Not Correct Trigger Point Drivers
Opioids may reduce pain temporarily, but they do not fix the biomechanical, neuromuscular, sleep, stress, or movement contributors that usually keep MPS active.
Tolerance, Dependence, and Addiction
Long-term opioid exposure can lead to tolerance, dependence, and misuse risk — all problematic in a condition that often needs active rehabilitation rather than escalating sedation.
Functional Impairment
Sedation, constipation, cognitive slowing, and reduced motivation can interfere with the exercise, physical therapy, and self-management strategies that are central to recovery.
Guidelines Generally Favor Non-Opioid Care
Most modern pain guidelines do not position opioids as a routine treatment for ordinary myofascial pain. They are generally viewed as poor fits for the long-term management of this condition.
The better alternative: multimodal pain management
Combine physical therapy and manual trigger point work with non-opioid pharmacotherapy (NSAIDs, muscle relaxants, TCAs/SNRIs), targeted injections when indicated, exercise and posture correction, stress management, and sleep optimization. This broader approach treats the underlying drivers rather than just masking symptoms.
Supportive Supplements
Supplements should be framed as supportive adjuncts when clinically relevant, not as automatic core treatment for all MPS patients.
Magnesium
ModerateMagnesium is often discussed in chronic pain because of its role in muscle function, sleep, and broader pain modulation.
Vitamin D
Moderate-StrongVitamin D status is often reviewed in persistent musculoskeletal pain, particularly when deficiency is suspected.
Omega-3 Fatty Acids (EPA/DHA)
ModerateOften discussed for inflammation-relevant pain and broader health support.
Turmeric / Curcumin
Limited to ModerateSometimes used as an anti-inflammatory adjunct, though product quality and formulation matter a great deal.
Coenzyme Q10 (CoQ10)
LimitedSometimes discussed when fatigue, statin use, or low energy states overlap with chronic pain.
Vitamin B12 (Methylcobalamin)
ModerateMost relevant when deficiency or neuropathic features are present.
Important Principles
Medications Are Adjuncts, Not Cures
Pharmacological treatment should support movement, rehabilitation, sleep, stress management, and symptom control — not replace them.
Every agent needs to fit your full medication list
All medications, supplements, and injections need review in the context of your health history, other medications, and treatment goals.
Individual Variation Is the Norm
Different patients respond very differently to the same medication. Trial, reassessment, and careful follow-up matter more than one-size-fits-all claims.
Start Low, Go Slow
A cautious, reassessed approach is usually safer and more clinically useful than starting aggressively.
Function and sleep, not just pain score
Pain, function, sleep, side effects, and day-to-day ability are often more useful than pain score alone when deciding whether a treatment is worth continuing.
Multimodal Is Usually Best
The strongest practical approach usually combines appropriate medication use with physical therapy, self-care, load management, and broader recovery work.