TrP 1
TrP1
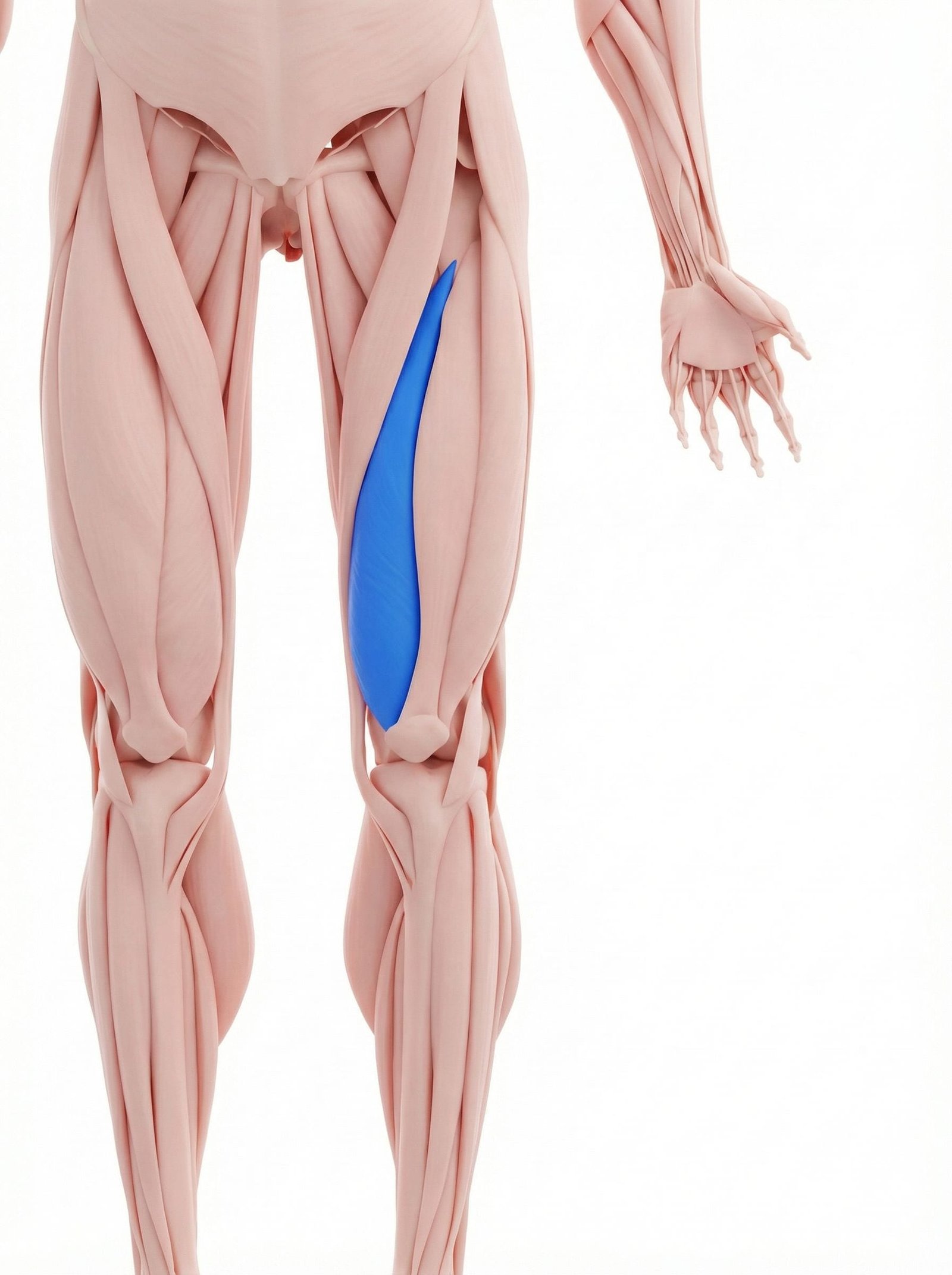
Location. Inner front thigh
Pain referral. Inner knee, inner thigh, knee cap
- Inner knee
- Inner thigh
- Knee cap
- Medial thigh
Medial knee aching from distal vastus medialis trigger point referral to joint line
Location. Inner front thigh
Pain referral. Inner knee, inner thigh, knee cap
Location. Distal fibers of VMO (vastus medialis oblique portion)
Pain referral. Deep inside the knee joint with knee buckling sensation
Inner knee pain. Medial knee aching from distal vastus medialis trigger point referral to joint line
Knee cap pain. Retropatellar or peripatellar aching from VMO dysfunction altering patellar tracking
Difficulty extending knee. Weak or painful terminal knee extension from vastus medialis oblique trigger point inhibition
Knee instability. Sense of knee giving way from VMO weakness reducing patellar stabilization medially
Deep internal knee pain. Distal VMO trigger point refers deep aching inside medial knee joint mimicking intra-articular pathology
Knee buckling or giving way. VMO inhibition from trigger point causes sudden quadriceps failure during weight-bearing activities
Knee instability sensation. Weakened VMO from trigger point impairs patellar tracking creating functional instability perception
Pain walking on uneven ground. Unstable surfaces demand VMO activation for knee control loading the inhibited trigger point
Locking sensation in knee. VMO trigger point dysfunction alters patellofemoral mechanics creating pseudo-locking catching sensation
Running. Repetitive knee extension demands during running fatigue vastus medialis with each stride
Squatting. Deep knee flexion loading eccentrically overloads vastus medialis especially in terminal range
Weak quadriceps. Insufficient VMO strength allows lateral patellar tracking increasing medial compartment stress
Patellar tracking issues. Abnormal patellar kinematics increase VMO demand as it attempts to correct tracking
Knee surgery. Post-surgical VMO inhibition from swelling leads to atrophy and compensatory trigger points
Overuse. Excessive repetitive knee extension activities fatigue vastus medialis beyond recovery capacity
Post-knee surgery (especially ACL reconstruction). Post-surgical VMO atrophy and reflex inhibition creates distal trigger points during recovery
Running with overpronation. Foot overpronation increases tibial internal rotation stressing VMO at oblique insertion angle
Weak VMO from disuse. Quadriceps deconditioning preferentially weakens VMO creating overload during reactivation
Patellar tracking problems. Lateral patellar tracking increases VMO demand for medial stabilization exceeding fiber capacity
Knee effusion or swelling. Joint effusion reflexively inhibits VMO through arthrogenic muscle inhibition creating trigger points
Prolonged immobilization. Extended knee immobilization causes VMO atrophy with trigger point formation upon resumed activity
Sit with your leg extended and relaxed. Using both thumbs, gently push the kneecap inward (medially), outward, up, and down. Hold each direction for 10 seconds. This improves patellar tracking and reduces pressure on the VMO trigger points.
Apply a warm heat pack to the inner aspect of the knee and lower inner thigh. This targets the VMO area directly. Combine with gentle knee bending and straightening while the heat is applied to improve circulation to the trigger point area.
Sit with a rolled towel under the affected knee. Straighten the knee fully by lifting the foot, focusing on the last 20-30 degrees of extension. Hold for 5 seconds at full lock-out, squeezing the inner quad. Lower slowly. This specifically targets the VMO.
Stand with a small ball between your knees. Bend your knees to about 30-45 degrees while squeezing the ball. Hold for 3 seconds, then straighten. The ball squeeze activates the VMO specifically, helping restore quadriceps balance.
Limit knee bend to 90 degrees or less during squats and lunges until symptoms improve. Use a railing when going downstairs. Avoid kneeling or sitting with legs folded underneath. Maintain a healthy weight to reduce knee joint loading.
If inner knee pain or knee instability persists beyond 3-4 weeks, consult a physiatrist or sports medicine physician. They can assess for meniscal injury, patellofemoral syndrome, or VMO atrophy and develop a comprehensive treatment plan including potential trigger point injection.