TrP 1
TrP1
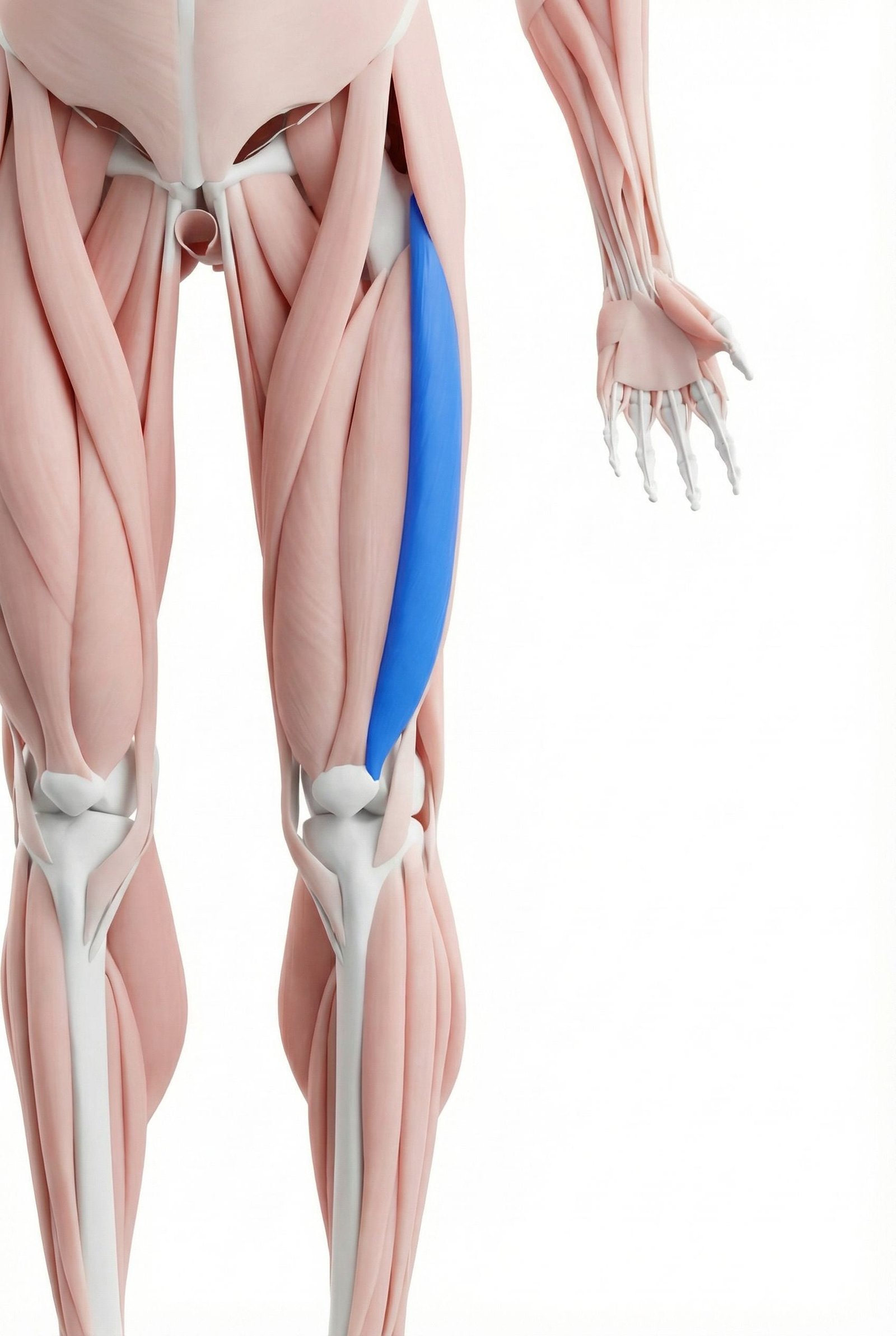
Location. Outer front thigh
Pain referral. Outer thigh, outer knee, hip
- Outer thigh
- Outer knee
- Hip
- Lateral thigh
Lateral thigh aching along the vastus lateralis belly worsened by walking or running
Location. Outer front thigh
Pain referral. Outer thigh, outer knee, hip
Location. Lateral knee, distal vastus lateralis near iliotibial band
Pain referral. Outer side of the knee
Location. Upper lateral thigh, proximal vastus lateralis near greater trochanter
Pain referral. Upper outer thigh and lateral hip region
Location. Mid-belly of vastus lateralis
Pain referral. Lateral thigh mimicking IT band syndrome
Location. Proximal vastus lateralis near greater trochanter
Pain referral. Lateral hip and lateral thigh
Outer thigh pain. Lateral thigh aching along the vastus lateralis belly worsened by walking or running
Outer knee pain. Lateral knee discomfort from distal vastus lateralis trigger point referral pattern
Difficulty extending knee. Painful or weak knee extension from trigger point inhibition of vastus lateralis
IT band-like symptoms. Lateral thigh tightness and knee pain mimicking iliotibial band friction syndrome
Lateral knee pain. Outer knee aching from distal vastus lateralis trigger points near the lateral retinaculum
Pain with patellar tracking. Lateral patellar deviation from vastus lateralis tightness pulling the patella outward
Knee stiffness after sitting. Theater sign stiffness from shortened distal vastus lateralis restricting patellar glide
Pain descending stairs. Lateral knee pain during eccentric quadriceps loading in stair descent from trigger points
Sensation of knee locking. Perceived catching from patellar maltracking caused by lateral vastus imbalance and tightness
Difficulty walking up stairs. Stair climbing requires eccentric quadriceps loading that stresses the proximal trigger point
Pain lying on the affected side. Lateral compression of proximal vastus lateralis against trochanter aggravates tender trigger point
Knee pain with prolonged sitting. Sustained knee flexion shortens quadriceps creating ischemia in trigger point region
Stiffness in the lateral thigh. Taut band in proximal vastus lateralis restricts tissue extensibility and lateral thigh mobility
Lateral thigh pain. Mid-belly vastus lateralis trigger point refers aching along lateral thigh paralleling IT band
IT band-like tightness. Taut vastus lateralis band creates lateral thigh tension mimicking IT band syndrome presentation
Difficulty lying on affected side. Lateral compression of mid-belly trigger point against femur during side-lying causes pain
Pain running and cycling. Repetitive quadriceps loading during running and cycling cyclically stresses mid-belly trigger point
Lateral hip pain. Proximal vastus lateralis trigger point refers to lateral hip mimicking trochanteric pathology
Greater trochanter tenderness. Referred tenderness at greater trochanter from proximal vastus lateralis periosteal irritation
Pain lying on side. Side-lying compresses proximal trigger point against greater trochanter causing nocturnal pain
Difficulty with hip abduction. Proximal trigger point tension restricts lateral thigh mobility impairing hip abduction range
Lateral thigh ache with walking. Gait-cycle quadriceps activation during stance phase loads proximal trigger point with each step
Running. Repetitive knee extension demand during running stride fatigues vastus lateralis each cycle
Cycling. Sustained concentric knee extension during pedaling overloads vastus lateralis progressively
Squatting. Deep knee flexion under load eccentrically overloads vastus lateralis muscle fibers
Weak quadriceps. Insufficient quadriceps strength increases vastus lateralis compensatory loading during activities
Poor biomechanics. Faulty knee tracking increases lateral quadriceps demand and vastus lateralis overactivation
Overuse. Excessive training volume without adequate recovery creates cumulative vastus lateralis fatigue
Running (especially downhill). Eccentric quadriceps loading during downhill running overloads distal vastus lateralis fibers
Squatting with poor form. Valgus knee collapse during squats increases lateral quadriceps loading and trigger point risk
IT band tightness. Iliotibial band restriction increases mechanical stress on adjacent distal vastus lateralis fibers
Weak hip abductors. Gluteal insufficiency causes compensatory vastus lateralis overactivation for lateral knee stability
Overuse in endurance sports. Cumulative lateral quadriceps loading in endurance activities creates persistent distal trigger points
Squatting (especially deep squats). Deep squat demands maximal vastus lateralis lengthening under load creating microtrauma
Climbing stairs repeatedly. Repetitive concentric quadriceps effort during stair ascent accumulates proximal fiber fatigue
Prolonged standing. Static quadriceps contraction to maintain knee extension causes sustained proximal fiber ischemia
Lateral lunges. Lateral lunge eccentrically loads vastus lateralis in frontal plane exceeding fiber tolerance
IT band syndrome compensation. Lateral thigh guarding from IT band pain creates secondary vastus lateralis mid-belly trigger points
Side-sleeping on hard mattress. Firm mattress compresses proximal vastus lateralis against trochanter creating ischemic trigger points
Weak hip stabilizers. Deficient hip abductor strength forces proximal vastus lateralis to compensate for pelvic stability
Post-total hip replacement. Surgical approach through lateral tissues creates scar and residual proximal trigger points
Hiking on rough terrain. Uneven terrain walking demands continuous proximal quadriceps stabilization creating overload
Lie on your side with a foam roller under the outer thigh. Roll slowly from the hip to just above the knee, pausing on tender spots for 20-30 seconds. Use your top leg placed in front for balance and to control how much body weight you place on the roller.
Stand and bend the affected knee, grabbing your ankle behind you. Pull the heel toward your buttock while keeping your knees close together. Tilt your pelvis forward slightly to increase the stretch along the outer quad. Hold a wall for balance.
Stand with your back against a wall, feet shoulder-width apart. Slide down until your knees are bent about 45-60 degrees. Hold this position while squeezing a small ball between your knees. This strengthens all quadriceps components in a balanced manner.
Stand on a step on the affected leg. Slowly lower the opposite foot toward the ground by bending the stance knee over 3-5 seconds. Tap the ground lightly, then push back up. This eccentrically loads the vastus lateralis, strengthening it while reducing trigger point sensitivity.
Increase running or cycling distance by no more than 10% per week. Use shoes with adequate lateral support and replace them regularly. Avoid deep squats until symptoms improve. Stretch quads after every exercise session.
If outer thigh or knee pain persists beyond 3-4 weeks, consult a physiatrist or sports medicine physician. They can differentiate vastus lateralis trigger points from IT band syndrome, lateral meniscus injury, or patellofemoral syndrome and provide targeted treatment.
Sit with the affected leg extended. Using your thumbs or a massage ball, apply sustained pressure to tender spots along the outer quadriceps just above the kneecap. Work slowly from about 4 inches above the kneecap down to the lateral patellar border, holding each tender point for 20-30 seconds.
Lie on your side with the foam roller under the outer thigh of the affected leg. Support yourself with your forearm and slowly roll from just above the knee to the hip. Pause on tender spots for 20-30 seconds. Cross the top leg in front for support to control pressure. Avoid rolling directly on the knee joint.
Stand on a step with the affected leg. Slowly lower the opposite foot toward the floor by bending the standing knee, taking 3-4 seconds to descend. Lightly tap the heel on the ground without fully transferring weight, then return to standing. Focus on keeping the knee aligned over the second toe.
Perform terminal knee extensions by placing a rolled towel under the affected knee while seated. Straighten the knee fully and hold for 5 seconds, squeezing the inner quad (VMO) at full extension. Also perform wall sits with a ball between the knees, squeezing gently to activate the VMO while maintaining the hold.
Apply a strip of rigid sports tape or kinesiology tape from the outer border of the patella, pulling gently toward the inner knee to encourage medial patellar glide. The tape should reduce lateral knee pain during activity. Reapply as needed. Consult a physical therapist for proper taping technique if unsure.
If lateral knee pain persists beyond 4-6 weeks of self-care, see an orthopedic specialist or sports medicine physician. They can assess for IT band syndrome, lateral meniscus pathology, lateral collateral ligament strain, or patellar maltracking using clinical tests and imaging such as MRI.
Lie on your side with the foam roller under your upper outer thigh. Support yourself with your forearm and slowly roll from just below the hip to mid-thigh, pausing on tender spots for 20-30 seconds. Avoid rolling directly over the bony greater trochanter.
Stand upright and cross the affected leg behind the opposite leg. Reach the arm on the affected side overhead and lean away from the affected side until you feel a stretch along the outer thigh and hip. Hold for 30 seconds and repeat.
Stand beside a step or low platform (6-8 inches high). Step up sideways with the affected leg, pressing through the heel and fully extending the knee and hip at the top. Lower slowly and repeat. Keep the pelvis level throughout.
Lie on your side with hips and knees bent at about 45 degrees, feet together. Keeping the feet touching, raise the top knee as high as possible without rotating the pelvis. Hold briefly, then slowly lower. Add a resistance band above the knees for progression.
Be mindful of sitting posture and avoid crossing the affected leg over the other. When sleeping, place a pillow between the knees to reduce lateral compression. Limit prolonged standing in one position by shifting weight or taking short walking breaks every 20-30 minutes.
If lateral thigh pain persists beyond 4-6 weeks of self-care, consult a sports medicine physician or physical therapist. They can assess for trochanteric bursitis, IT band pathology, or hip joint involvement and provide targeted manual therapy or imaging as needed.