TrP 1
TrP1
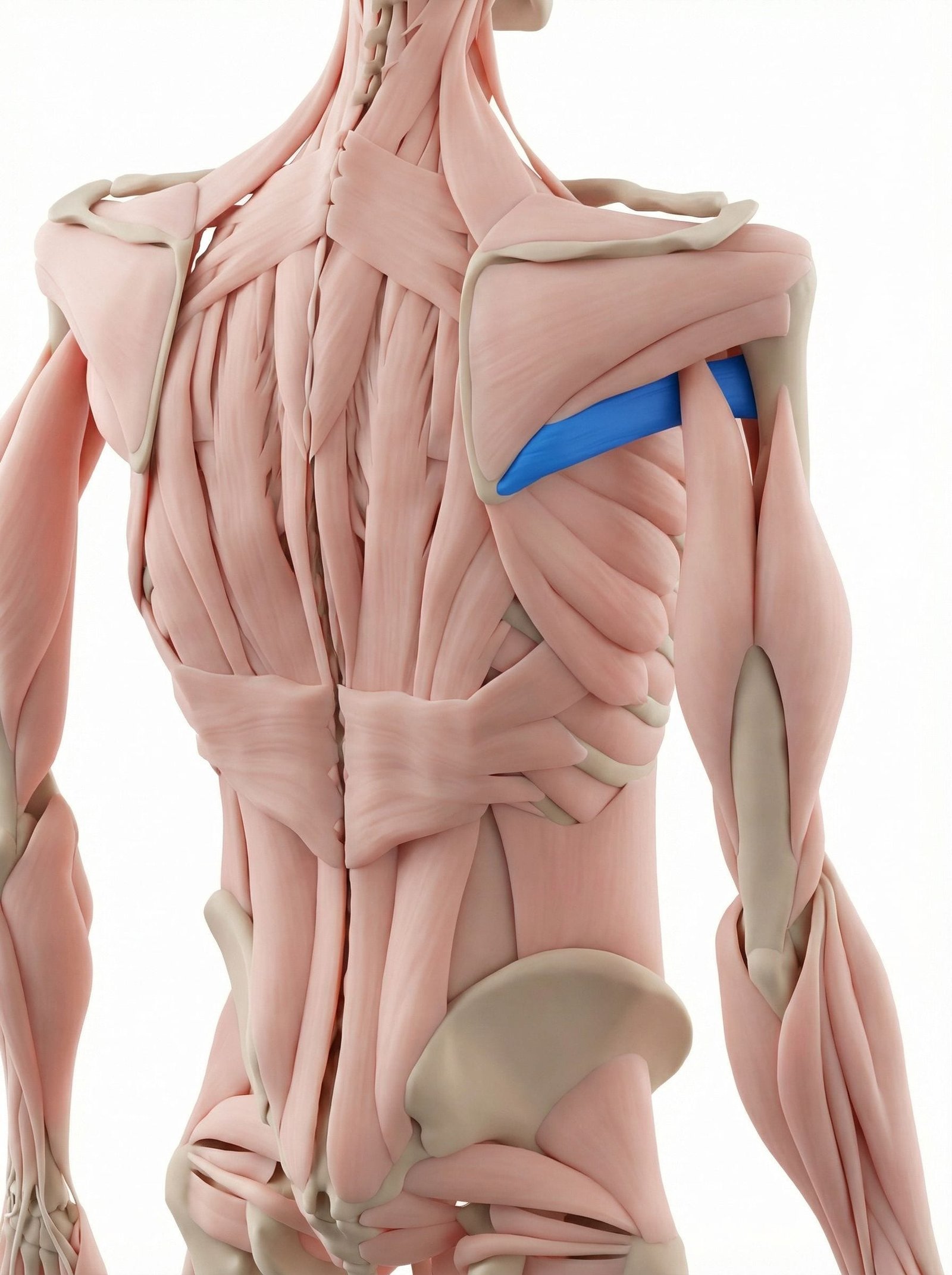
Location. Lower back of shoulder blade
Pain referral. Back of shoulder, posterior arm
- Back of shoulder
- Posterior arm
- Deltoid area
Deep aching behind shoulder from teres major trigger points at inferior scapular angle
Location. Lower back of shoulder blade
Pain referral. Back of shoulder, posterior arm
Location. Near inferior angle of scapula
Pain referral. Posterior shoulder and medial upper arm
Location. Near humeral insertion of teres major
Pain referral. Posterior deltoid region and medial upper arm
Posterior shoulder pain. Deep aching behind shoulder from teres major trigger points at inferior scapular angle
Arm pain. Referred pain traveling distally along posterior arm from shoulder trigger point activation
Difficulty with internal rotation. Restricted shoulder internal rotation from teres major trigger point taut band shortening
Deep aching in posterior shoulder. Teres major trigger points at the inferior scapular angle create deep posterior shoulder aching
Pain reaching overhead. Overhead reach stretches the teres major provoking trigger points at the inferior scapular attachment
Difficulty reaching behind back. Combined shoulder extension and internal rotation loads taut teres major bands creating restriction
Posterior axillary fold tenderness. Taut bands in the posterior axillary fold create palpable tenderness in the teres major belly
Restricted shoulder flexion and abduction. Teres major taut bands resist shoulder elevation limiting flexion and abduction range
Posterior shoulder pain with internal rotation. Teres major trigger point pain during internal rotation from maximal muscle shortening contraction
Medial upper arm ache. Referred pain along medial proximal arm from teres major trigger point near humeral insertion
Difficulty reaching overhead. Shortened teres major restricts shoulder flexion needed for full overhead reaching range
Pain with latissimus-type movements. Pulling and adduction movements co-activate teres major aggravating insertion trigger points
Pulling exercises. Repetitive shoulder extension and adduction during pull-ups overloads teres major fibers
Swimming. Pull-through phase of swim strokes creates repetitive teres major loading each cycle
Throwing. Deceleration phase of throwing demands forceful eccentric teres major contraction repeatedly
Overhead activities. Sustained or repetitive overhead reaching overloads teres major during arm lowering phases
Repetitive pulling motions (rowing, climbing). Pulling movements maximally load the teres major as a shoulder extensor and internal rotator
Chronic shoulder internal rotation. Sustained internal rotation posture shortens the teres major creating chronic ischemic trigger points
Carrying heavy bags on one shoulder. Sustained scapular depression with heavy loads overloads the teres major at its inferior attachment
Lat pulldown exercises with excessive weight. Heavy lat pulldowns demand maximal teres major activation as a synergist to latissimus dorsi
Compensating for weak rotator cuff. Rotator cuff insufficiency transfers stabilization demands to the teres major creating overload
Lat pulldowns and rows. Repetitive pulling exercises overload teres major as a shoulder adductor and internal rotator
Swimming (pull phase). Aquatic pulling phase maximally loads teres major through adduction and internal rotation
Rock climbing. Sustained pulling and shoulder adduction during climbing overloads teres major chronically
Pulling heavy objects. Forceful pulling creates high concentric loads on teres major at its humeral insertion
Post-shoulder surgery adhesions. Surgical adhesions restrict teres major mobility creating compensatory trigger points at insertion
Stand with your back to a wall and place a tennis ball between your body and the wall at the back of your shoulder near the armpit area (lower scapula border). Lean into the ball with moderate pressure and slowly roll it around to find tender spots. When you find a sore point, hold sustained pressure for 20-30 seconds until you feel the tenderness ease.
Stand in a doorway and raise the affected arm overhead, grasping the doorframe with your hand. Step forward slightly with the same-side foot, allowing your body to shift forward and to the opposite side. You should feel a deep stretch along the back of your shoulder and down the side of your torso. Keep your core engaged and avoid arching your lower back.
Attach a resistance band at elbow height to a doorknob or sturdy anchor. Stand with your affected side toward the anchor, elbow bent 90 degrees and tucked against your side. Rotate your forearm inward across your body against the band resistance. Control the movement slowly in both directions. Keep your elbow pinned to your side throughout.
Using a resistance band anchored at chest height, sit upright and pull the band toward your lower chest, squeezing your shoulder blades together at the end of each pull. Focus on controlled retraction rather than heavy resistance. Keep shoulders down and away from ears throughout the movement.
Avoid sleeping on the affected side, as this compresses the teres major against the mattress. If you sleep on your back, place a small pillow under the affected arm to keep it slightly elevated. If you sleep on the opposite side, hug a pillow to prevent the affected arm from rolling forward and internally rotating.
If posterior shoulder pain persists beyond 3-4 weeks of self-care, consult a physiotherapist or orthopedic specialist. They can differentiate teres major trigger points from rotator cuff tears, labral injuries, or thoracic outlet issues through specific clinical tests and imaging if needed. Targeted manual therapy and dry needling can be highly effective for persistent teres major trigger points.