TrP 1
TrP1
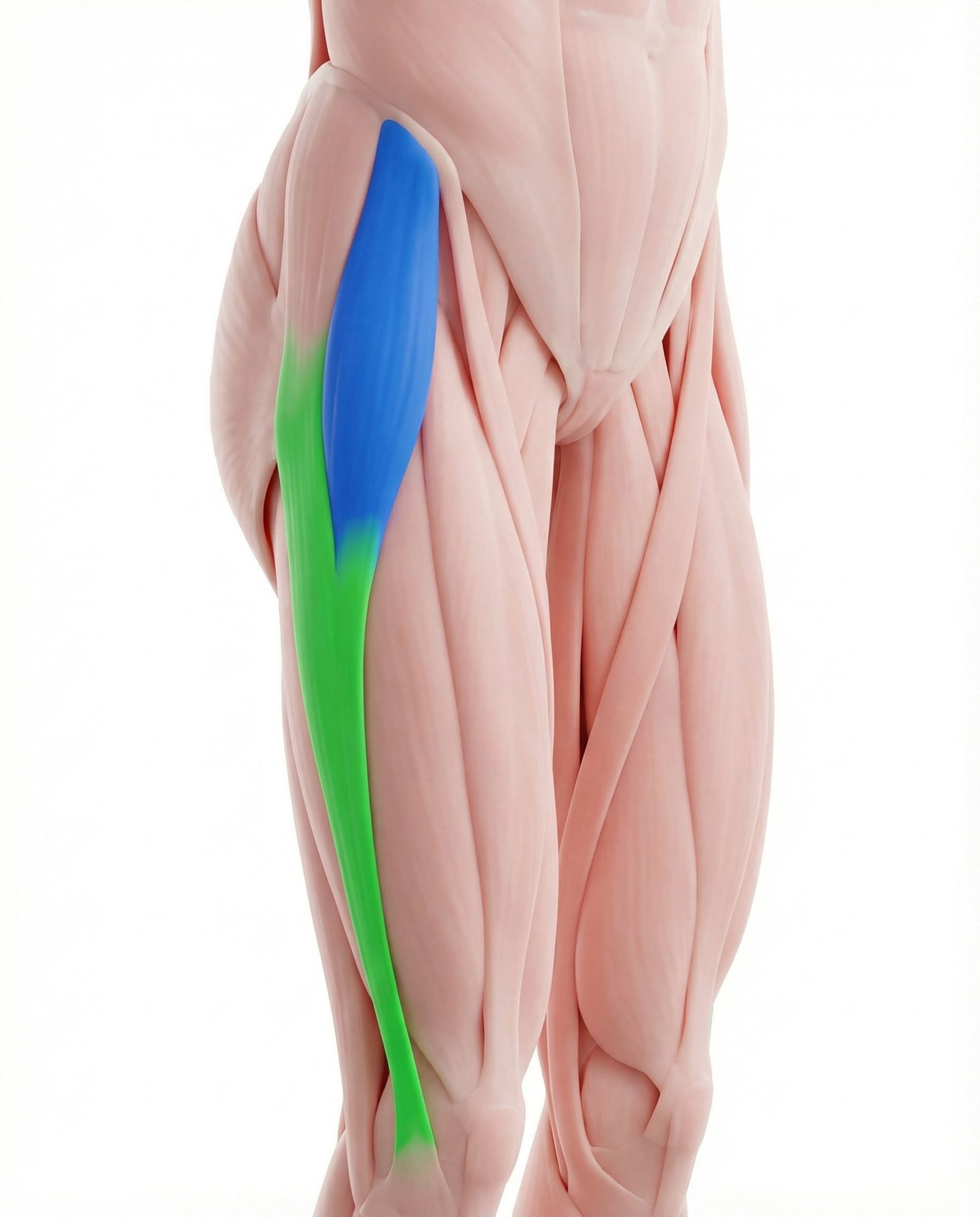
Location. Front/side of hip
Pain referral. Front of hip, outer thigh, knee
- Front of hip
- Outer thigh
- Outer knee
- Buttock
Anterolateral hip aching near the ASIS from TFL trigger point tension and referral
Location. Front/side of hip
Pain referral. Front of hip, outer thigh, knee
Location. Lateral thigh at the junction of TFL muscle belly and iliotibial band
Pain referral. Outer thigh and lateral knee
Location. Distal TFL near ITB junction
Pain referral. Lateral thigh and lateral knee along IT band
Location. Posterior fibers near gluteal attachment
Pain referral. Lateral hip and greater trochanter region
Hip pain. Anterolateral hip aching near the ASIS from TFL trigger point tension and referral
Outer thigh pain. Lateral thigh aching along the iliotibial band from TFL trigger point radiation
Knee pain. Lateral knee discomfort from IT band tension transmitted by hypertonic TFL muscle
IT band tightness. Palpable lateral thigh tautness from TFL tension transmitted through the iliotibial band
Difficulty walking. Antalgic gait pattern from anterolateral hip pain during swing and stance phases
Lateral thigh pain. Aching along iliotibial band from distal TFL trigger point tension transmitted distally
Outer knee pain. IT band tension from TFL trigger point creates friction and pain at lateral femoral condyle
Hip pain on the side. Lateral hip aching from trigger point proximity to greater trochanter and trochanteric bursa
Pain with walking or running. Repetitive IT band excursion over lateral knee during gait irritates sensitized tissues
Snapping sensation at the hip. Taut TFL band snaps over greater trochanter during hip flexion and extension cycles
Lateral knee ache. Referral extends distally along the IT band to the lateral femoral condyle and Gerdy tubercle
Snapping hip (lateral). Increased IT band tension from TFL trigger points causes audible snapping over the greater trochanter
Pain lying on affected side. Lateral recumbent position compresses the greater trochanter against taut IT band and TFL
Lateral hip pain mimicking trochanteric bursitis. Greater trochanter region ache from TFL trigger point referral simulating bursal inflammation
Greater trochanter tenderness. Palpable tenderness over greater trochanter from TFL taut band tension at lateral hip
Pain with hip abduction. Active hip abduction contracts TFL aggravating trigger points near posterior gluteal attachment
Running. Repetitive hip flexion and abduction during running stride fatigues TFL each gait cycle
Walking. Prolonged walking demands sustained TFL activation for hip stabilization during stance
Weak glutes. Insufficient gluteal strength forces TFL to compensate as hip abductor and stabilizer
Tight hip flexors. Hip flexor shortening increases TFL workload as compensatory flexion-abduction stabilizer
Poor biomechanics. Faulty lower extremity alignment increases TFL compensatory activation during gait
Prolonged sitting. Sustained hip flexion shortens TFL adaptively creating chronic taut band formation
Running (especially on banked surfaces). Cambered running surfaces create asymmetric hip abductor loading overworking downhill TFL
Cycling. Repetitive hip flexion with internal rotation bias chronically activates TFL during pedaling
Weak gluteus medius. TFL compensates for insufficient gluteus medius hip abduction and stabilization capacity
Poor running biomechanics. Excessive hip adduction and internal rotation during stance phase overloads TFL
Prolonged standing on one leg. Unilateral stance demands sustained TFL contraction for frontal plane pelvic stability
Hiking downhill. Eccentric TFL loading during downhill descent with repetitive braking stresses muscle fibers
Hiking (downhill). Downhill hiking increases eccentric TFL and IT band loading during each deceleration step
Weak hip abductors. Insufficient gluteus medius strength forces TFL to compensate as a secondary hip abductor
Standing on one leg habitually. Single-leg stance demands continuous TFL contraction for frontal plane pelvic stabilization
Limping from injury (compensatory). Antalgic gait alters hip mechanics increasing compensatory TFL recruitment on the unaffected side
Running (especially on cambered surfaces). Cambered surface running creates asymmetric TFL loading as it stabilizes the pelvis laterally
Lateral hip muscle weakness. Weak gluteus medius shifts lateral hip stabilization demand to TFL causing compensatory overload
IT band syndrome compensation. TFL overworks to compensate for IT band friction syndrome altering lateral hip biomechanics
Sleeping on affected side. Sustained lateral hip compression during side-lying creates positional TFL trigger points
Standing on one leg frequently. Habitual single-leg stance overloads ipsilateral TFL as a primary pelvic stabilizer
Lie on the affected side with a foam roller under your outer thigh, from the hip down toward the knee. Roll slowly along the length of the IT band and TFL. When you find a particularly tender spot, hold for 20-30 seconds. Support yourself with your hands and opposite foot to control pressure.
Stand next to a wall for balance. Cross the affected leg behind the opposite leg. Lean your hip toward the wall on the affected side while reaching the arm on the same side overhead and away from the wall. You should feel a stretch on the front-outer hip.
Lie on the non-affected side with hips and knees bent to about 45 degrees, feet together. Keeping your feet together, lift the top knee as high as possible without rotating your pelvis. Hold for 3 seconds, then lower slowly. This activates the gluteus medius, reducing compensatory TFL overuse.
In a half-kneeling position (one knee down), shift your weight forward while keeping your trunk upright. Then lean slightly away from the kneeling side to add a lateral stretch component that specifically targets the TFL. Hold for 30 seconds.
Use well-cushioned running shoes and replace them every 400-500 miles. Increase running distance by no more than 10% per week. Avoid running on cambered surfaces that load one side more than the other. When sleeping, avoid lying on the affected side or use a pillow between your knees.
If lateral hip or thigh pain persists beyond 3-4 weeks, consult a physiatrist. They can differentiate between TFL trigger points, trochanteric bursitis, and IT band friction syndrome, and provide targeted treatment. A gait analysis may also reveal biomechanical factors contributing to TFL overload.
Lie on your side with a foam roller under the lateral thigh between the hip and knee. Support your body weight with your forearm and opposite foot. Slowly roll from the hip down to just above the knee, pausing on tender spots for 20-30 seconds. Avoid rolling directly over the bony prominence of the hip or knee.
Stand next to a wall for balance. Cross the affected leg behind the other leg. Shift your hips toward the affected side while leaning your upper body away, creating a stretch along the outer hip and lateral thigh. Keep both feet on the ground. Hold for 30 seconds.
Lie on your unaffected side with both legs straight. Keeping the top leg straight and toes pointing forward, slowly lift it to about 30-40 degrees. Hold briefly at the top, then lower under control. Avoid rolling the pelvis backward. Progress by adding an ankle weight.
Stand on the affected leg on a step or flat surface. Slowly bend the knee to about 30-40 degrees while keeping the pelvis level and the knee tracking over the second toe. Avoid letting the hip drop on the non-stance side. Slowly return to standing.
Run on flat, even surfaces rather than cambered roads. Alternate running direction on tracks. Shorten your stride slightly to reduce hip adduction angle. Ensure running shoes provide adequate lateral support. Consider a gait analysis if lateral hip or knee pain recurs with running.
If lateral thigh and knee pain persists beyond 4-6 weeks despite stretching and strengthening, consult a physical therapist or sports medicine specialist. They can perform instrument-assisted soft tissue mobilization, dry needling of the distal TFL, gait analysis, and rule out trochanteric bursitis or lateral meniscus pathology.