TrP 1
TrP1
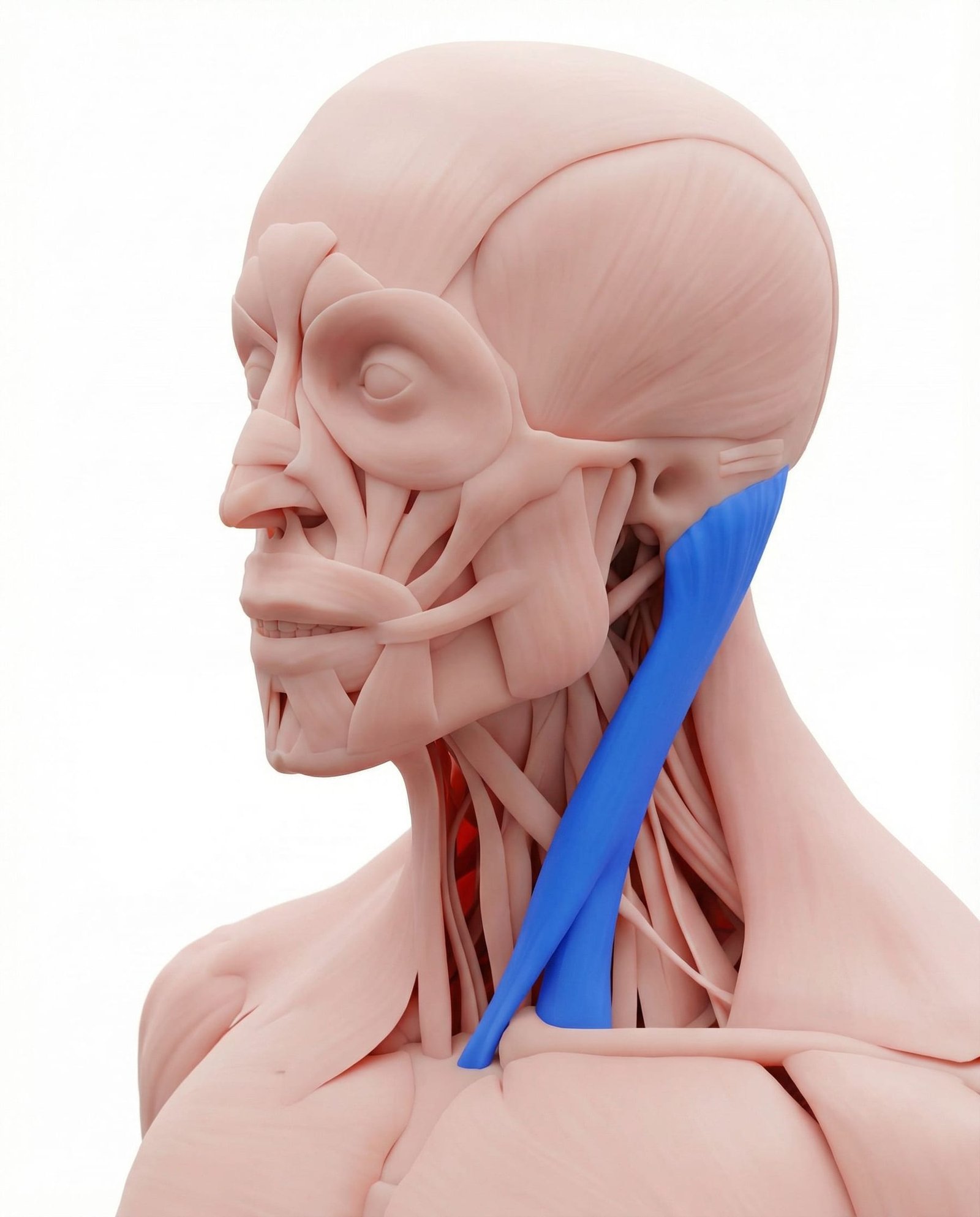
Location. Front of neck, from sternum to mastoid
Pain referral. Front and side of neck, head
- Front of head
- Behind eye
- Top of head
- Ear
- Back of head
- Cheek
- Throat
Tension-type or migraine-like pain from trigger point referred pain patterns
Location. Front of neck, from sternum to mastoid
Pain referral. Front and side of neck, head
Location. Lower lateral head, clavicular division of sternocleidomastoid
Pain referral. Side of face, ear, and forehead
Location. Lower sternal head of SCM near sternal attachment
Pain referral. Throat, sternum, and sternal notch
Location. Upper sternal head of SCM near mastoid process insertion
Pain referral. Cheek, malar (zygomatic) region, and jaw
Location. Mid-clavicular head of SCM
Pain referral. Forehead bilaterally and deep ear pain
Headache. Tension-type or migraine-like pain from trigger point referred pain patterns
Dizziness. Vestibular disturbance from trigger point compression of proprioceptive pathways
Blurred vision. Visual disturbance from referred autonomic effects of active trigger points
Ear pain. Deep otalgia referred from SCM sternal division without middle ear pathology
Neck pain. Anterior and lateral cervical aching worsened by rotation and head turning
Facial pain. Referred pain to cheek and periorbital area mimicking sinus or dental origin
Frontal headache. Bilateral frontal aching from SCM clavicular division trigger points referring to the forehead
Ear pain (deep). Deep otalgia from clavicular SCM trigger points referring to the inner ear region
Dizziness or spatial disorientation. Vestibular-like symptoms from SCM trigger points disrupting cervical proprioceptive input pathways
Tearing of the eye. Ipsilateral lacrimation from autonomic effects of SCM clavicular trigger point activation
Sinus-like congestion feeling. Perceived nasal congestion from SCM referral to maxillary area without actual sinus inflammation
Sore throat without infection. SCM sternal trigger point refers pain to pharyngeal region mimicking infectious pharyngitis
Sternal discomfort. Referred pain to sternum and sternal notch from lower SCM attachment trigger point
Sensation of throat tightness. Referred tension to anterior cervical structures creates globus-like throat constriction feeling
Difficulty swallowing sensation. Referred pharyngeal discomfort creates subjective dysphagia without structural obstruction
Anterior neck ache. Localized aching along anterior cervical triangle from sternal SCM trigger point irritation
Cheek pain. SCM sternal TrP3 refers pain to malar region via trigeminal nerve convergence pathways
Jaw ache mimicking dental issues. Referred mandibular pain from SCM trigger point creates false impression of dental pathology
Facial pain on one side. Unilateral facial aching from ipsilateral SCM trigger point referral to zygomatic region
Pain around the eye socket. Supraorbital referred pain from upper SCM sternal trigger point mimicking orbital pathology
Toothache in upper jaw without dental cause. Referred maxillary tooth pain from SCM trigger point converging on trigeminal V2 territory
Bilateral frontal headache. Clavicular SCM trigger point uniquely refers pain bilaterally across frontal bone region
Deep ear pain. Referred otalgia from clavicular SCM through auricular branch nerve convergence pathways
Ear stuffiness sensation. SCM trigger point influences eustachian tube tension creating subjective aural fullness
Spatial disorientation. Altered cervical proprioception from SCM trigger point disturbs vestibular-cervical integration
Lacrimation on affected side. Autonomic reflex stimulation from SCM trigger point activates ipsilateral lacrimal secretion
Forward head posture. Chronic anterior head carriage increases mechanical load causing sustained contraction
Whiplash. Sudden cervical acceleration-deceleration injury creates acute muscle fiber damage
Stress. Psychological tension causes sustained involuntary muscle contraction and ischemia
Shallow breathing. Accessory breathing pattern overworks SCM as a respiratory elevator muscle
Sleeping with poor neck support. Sustained awkward cervical positioning during sleep strains SCM fibers overnight
Reading in bed. Prolonged cervical flexion while propped up overloads the SCM concentrically
Prolonged computer work. Forward head position at desk sustains SCM contraction for extended periods
Stress and emotional tension. Chronic anxiety activates SCM through accessory breathing and cervical guarding reflex patterns
Paradoxical breathing. Upper chest breathing recruits SCM as accessory inspiratory muscle causing chronic overuse fatigue
Prolonged head turning. Sustained unilateral cervical rotation maintains SCM in shortened contracted position creating ischemia
Sleeping in prone position. Sustained extreme cervical rotation during prone sleeping overloads SCM unilaterally overnight
Chronic coughing. Repeated forceful neck flexion during coughing overloads SCM sternal head fibers
Whiplash injury. Rapid cervical flexion-extension damages SCM sternal attachment creating post-traumatic trigger points
Mouth breathing. Chronic mouth breathing alters head position increasing SCM sternal division demand
Sleeping with head flexed forward. Sustained neck flexion shortens SCM sternal fibers in sleeping position causing trigger points
Prolonged neck flexion from reading in bed. Sustained head-forward reading position overloads SCM sternal division isometrically
Chronic neck rotation to one side. Sustained unilateral rotation shortens ipsilateral SCM creating trigger points at insertion
Sleeping on stomach with head rotated. Prolonged maximal cervical rotation during sleep strains upper SCM sternal division
Stress-related jaw clenching. Concurrent jaw clenching and neck tension co-activate SCM and masticatory muscles
Prolonged phone use holding neck in flexion. Sustained neck flexion looking at phone overloads upper SCM fibers isometrically
Chronic upper chest breathing. Accessory breathing pattern recruits clavicular SCM as respiratory muscle causing overuse
Sleeping with neck twisted. Prolonged cervical rotation during sleep strains clavicular SCM fibers asymmetrically
Heavy helmet or headgear use. Added head weight from helmet increases clavicular SCM demand for cervical stabilization
Prolonged reading with neck in flexion. Sustained neck flexion for reading chronically loads clavicular SCM in shortened position
Turn your head slightly toward the side you want to treat to slacken the muscle. Grasp the SCM between your thumb and fingers — it is the prominent cord-like muscle on the side of the neck. Gently pinch and roll along its length from just below the ear down to the collarbone. When you find a tender nodule, hold gentle pressure for 20-30 seconds. Work slowly and carefully.
Apply a warm, damp towel or a microwaveable neck wrap to the side of the neck. The heat should cover from below the ear to the collarbone along the SCM. Lie down or sit comfortably with your head supported while applying. Combine with slow, deep breathing to enhance relaxation.
Sit upright with shoulders relaxed. Slowly turn your head to look over your right shoulder as far as comfortable, hold for 15-20 seconds. Return to center slowly, then repeat to the left. Keep the movement smooth and pain-free. Perform 5 repetitions to each side. If you feel dizziness during the stretch, slow down further or reduce the range.
Sit or stand tall with your shoulders back. Without tilting your head up or down, draw your chin straight back as if making a double chin. Hold for 5-10 seconds, feeling a gentle stretch at the base of the skull. Release and repeat. This strengthens the deep neck flexors and counteracts forward head posture, which overloads the SCM.
Position your computer monitor so the top of the screen is at eye level and about an arm's length away. When using your phone, bring it up to eye level instead of looking down. Avoid reading in bed with your head propped forward. Set up your car headrest so it contacts the back of your head, not the back of your neck.
Never hold a phone between your ear and shoulder — this intensely contracts the SCM and upper trapezius. Use speakerphone, a headset, or earbuds for all calls longer than 1 minute. If you frequently take calls at a desk, invest in a quality headset that you can wear comfortably for extended periods.
If you experience persistent dizziness, balance problems, visual disturbances, or ear symptoms that do not improve within 2-3 weeks of self-care, consult a physiatrist or neurologist. SCM trigger points can mimic serious conditions including vestibular disorders and cervicogenic vertigo. A professional can perform targeted trigger point therapy and rule out other causes.
Turn your head slightly toward the affected side to slacken the muscle. Grasp the lower portion of the SCM between your thumb and fingers just above the collarbone. Gently squeeze and roll the muscle belly, searching for tender taut bands. Apply gentle sustained pressure on any tender spots for 10-15 seconds, then release. Use only light to moderate pressure — the SCM is a superficial muscle and does not require deep force.
Apply a warm, moist towel or microwaveable heat wrap to the side of the neck over the SCM muscle. The warmth should be comfortable, not hot. Lie on your back with a small rolled towel under the neck curve for support while applying the heat. This increases blood flow to the muscle, helping to reduce trigger point irritability and associated autonomic symptoms like ear pain and tearing.
Sit upright in a chair. To stretch the left SCM clavicular division, place your left hand behind your back or under your left thigh. Tilt your right ear toward your right shoulder, then gently rotate your chin slightly upward and to the left. You should feel a stretch along the left side of the neck from the collarbone upward. Hold the position gently without bouncing. Repeat on the opposite side.
Sit or stand with your spine upright. Without tilting your head up or down, gently draw your chin straight back as if making a double chin. Hold for 5 seconds, then relax. Imagine a string pulling the back of your head upward and backward. This exercise corrects forward head posture, which is the primary perpetuating factor for SCM trigger points, by strengthening the deep cervical flexors and reducing SCM overload.
Place one hand on your chest and one on your abdomen. Breathe in through your nose, directing the breath into your belly so that your lower hand rises while your upper hand stays relatively still. Exhale slowly through pursed lips. Practice this pattern until it becomes habitual. Paradoxical (upper chest) breathing chronically overloads the SCM as an accessory inspiratory muscle, so restoring proper diaphragmatic breathing is essential to preventing recurrence.
If frontal headaches, ear pain, dizziness, or facial symptoms persist beyond 3-4 weeks of self-care, consult a physical therapist or manual therapist experienced in cervical myofascial pain. SCM trigger points can be secondary to upper cervical joint dysfunction, thoracic outlet syndrome, or vestibular disorders that require professional differential diagnosis. Skilled manual release of the SCM combined with postural retraining provides the most effective long-term outcomes.