TrP 1
TrP1
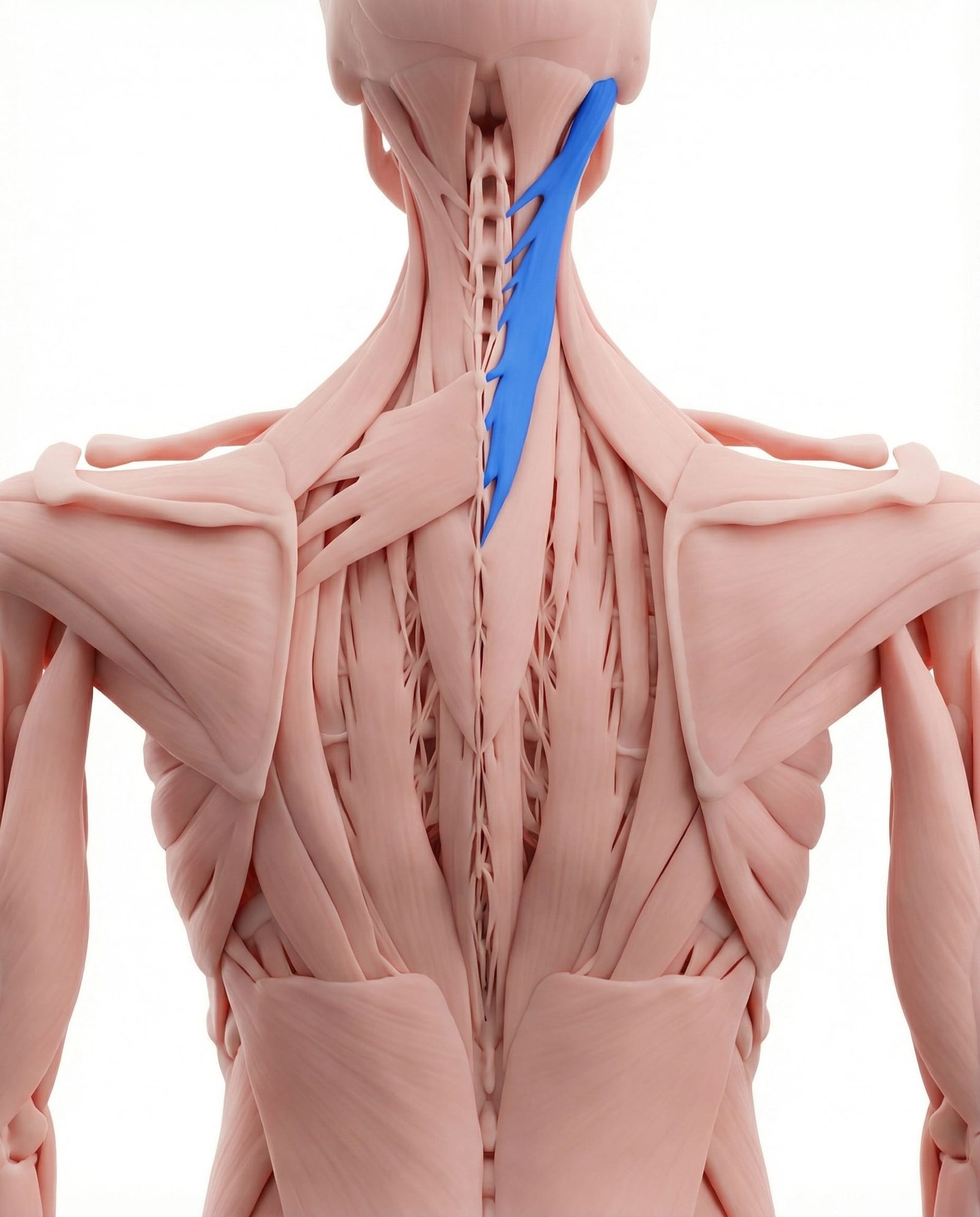
Location. Back of neck, upper cervical
Pain referral. Back of head, top of head
- Back of head
- Top of head
- Behind eye
- Neck
Occipital aching that radiates superiorly from splenius capitis trigger point referral
Location. Back of neck, upper cervical
Pain referral. Back of head, top of head
Location. Near mastoid insertion of splenius capitis
Pain referral. Top of head (vertex headache)
Location. Mid-belly of splenius capitis at C2-C3 level
Pain referral. Behind the eye and into the orbit (periorbital)
Headache at back of head. Occipital aching that radiates superiorly from splenius capitis trigger point referral
Pain at vertex. Top-of-head pain referred along the occipital nerve path to the cranial vertex
Neck stiffness. Restricted cervical extension and rotation from taut bands in posterior cervical muscles
Top of head headache. Splenius capitis mastoid trigger points refer superiorly to the vertex of the skull
Vertex pressure. Referred pain creates a pressure sensation at the crown mimicking intracranial pathology
Scalp tenderness at crown. Central sensitization from trigger point referral increases pericranial tissue sensitivity at vertex
Headache worse with neck movement. Cervical rotation and extension load the splenius capitis intensifying vertex-referred headache
Feeling of tight cap on head. Bilateral referral to the vertex creates a circumferential pressure sensation resembling a tight cap
Pain behind the eye. Mid-belly splenius capitis trigger points at C2-C3 refer anteriorly through the skull to the orbit
Retro-orbital ache. Convergent referral pathways project deep aching into the retro-orbital space behind the eye
Blurred vision (transient). Periorbital trigger point referral may cause autonomic disturbance affecting transient visual focus
Eye strain sensation. Referred orbital pain creates a perception of eye fatigue mimicking visual strain from screen work
Headache centered behind one eye. Unilateral splenius trigger points create a focused retro-orbital headache pattern on the affected side
Forward head posture. Anterior head carriage eccentrically overloads splenius capitis as it resists head flexion
Whiplash. Sudden cervical hyperextension acutely strains splenius capitis during deceleration injury
Sleeping position. Sustained cervical rotation during sleep overloads splenius capitis on one side
Stress. Emotional tension causes sustained posterior cervical muscle guarding and contraction
Computer work. Prolonged forward head position at desk increases splenius capitis stabilization demand
Sleeping in draft or cold air. Cold exposure causes reflexive cervical muscle contraction activating latent splenius trigger points
Whiplash injury. Rapid cervical acceleration-deceleration overloads splenius capitis creating traumatic trigger points
Prolonged reading with head down. Sustained cervical flexion eccentrically loads splenius capitis creating fatigue-induced trigger points
Stress and tension. Psychogenic cervical muscle tension chronically activates splenius capitis trigger points
Cold wind exposure on neck. Cold air on the posterior neck triggers reflexive splenius capitis contraction and trigger point activation
Computer screen glare. Squinting from screen glare increases facial and cervical tension activating splenius trigger points
Prolonged reading. Sustained cervical flexion during reading eccentrically overloads splenius capitis mid-belly fibers
Stress-related neck tension. Psychogenic cervical muscle guarding chronically activates splenius capitis trigger points at C2-C3
Poor pillow support during sleep. Inadequate cervical support during sleep maintains splenius capitis in a shortened or strained position
Stand with your back against a wall and place a tennis ball between the wall and the muscles at the base of your skull, just to one side of the spine. Lean your body weight gently into the ball and hold pressure on tender spots for 30-60 seconds. Slowly roll the ball along the base of the skull to find other tender areas. Keep your knees slightly bent to control the pressure.
Drape a warm, damp towel or microwavable heat wrap across the back of your neck and base of the skull. Lie on your back with the heat pack cradling your neck, or sit in a reclined position. The warmth should be comfortably hot but not burning. Close your eyes and breathe slowly to enhance relaxation.
Sit or stand tall with your shoulders relaxed. Draw your chin straight back, creating a double chin, without tilting your head up or down. Hold this retracted position for 5 seconds, then relax. You should feel a gentle stretch at the back of your neck and a mild activation of the deep neck muscles. Repeat for the prescribed number of repetitions.
Sit upright with your shoulders relaxed. Slowly turn your head to one side as far as comfortable, keeping your chin level. Hold the end position for 15-20 seconds, feeling a gentle stretch in the opposite side of the neck. Return to center slowly, then repeat to the other side. Avoid forcing the movement or bouncing at the end range.
Position your computer monitor so the top of the screen is at or just below eye level, preventing sustained neck extension or flexion. If you use a laptop, consider a separate monitor or a laptop stand with an external keyboard. Avoid reading or using devices while lying in bed, as this forces the neck into awkward flexion angles that strain the splenius capitis. Use a book stand or tablet holder at your desk instead.
If your headaches at the back or top of the head persist despite 2-3 weeks of consistent self-care, schedule an appointment with a physical therapist or headache specialist. Describe the location and pattern of your headaches, noting that the pain starts at the base of the skull. A professional can perform targeted manual therapy to the splenius capitis and rule out occipital neuralgia or other causes.