TrP 1
TrP1
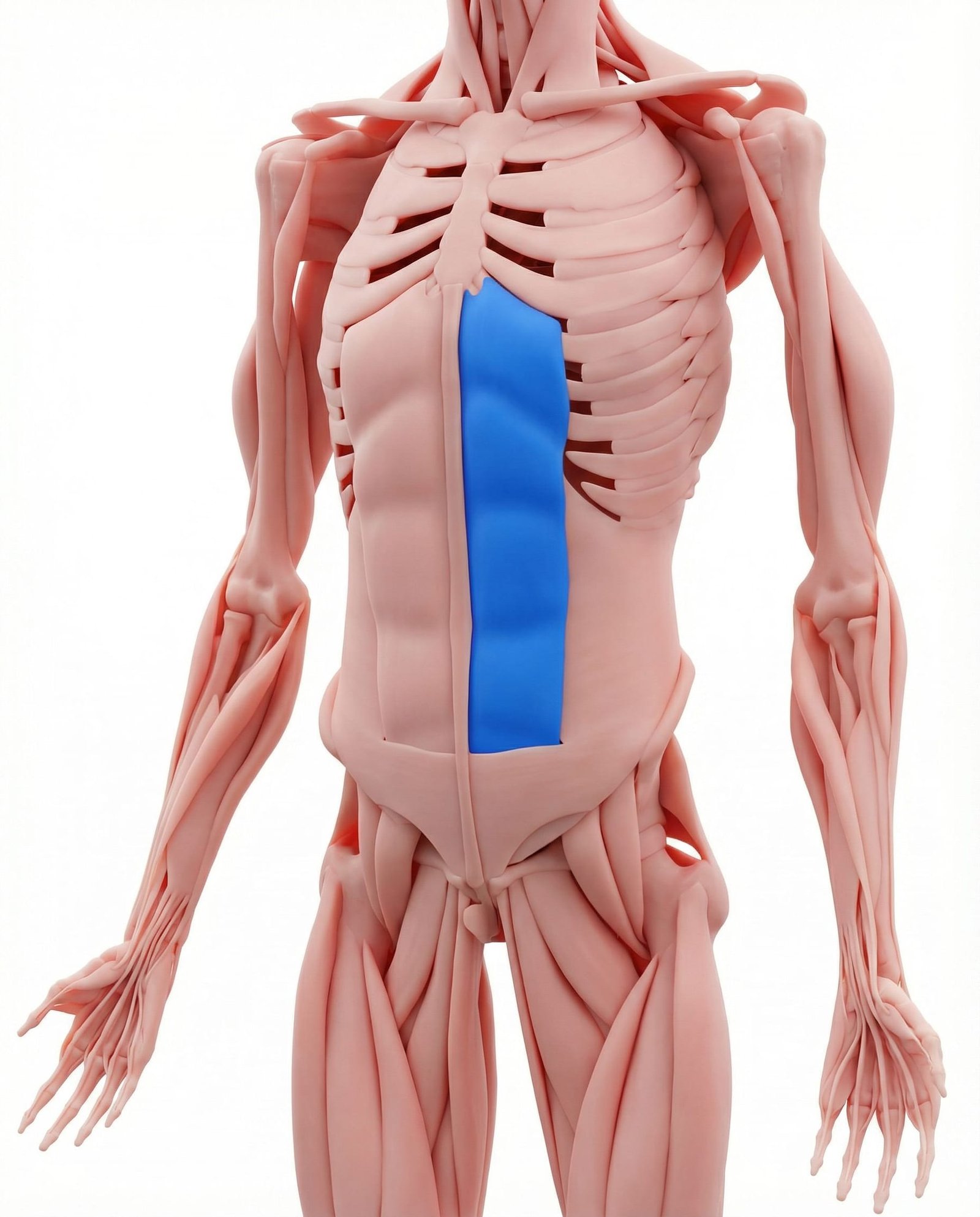
Location. Front of abdomen (six-pack area)
Pain referral. Midline abdomen, lower sternum, pubic area
- Midline abdomen
- Lower sternum
- Pubic area
- Across lower back
Midline abdominal aching that may mimic visceral pain from rectus trigger referral
Location. Front of abdomen (six-pack area)
Pain referral. Midline abdomen, lower sternum, pubic area
Location. Lower fibers near pubic symphysis
Pain referral. Lower abdomen and suprapubic region
Location. Upper fibers near xiphoid process
Pain referral. Epigastric region and bilateral mid-back
Location. Periumbilical region at mid-belly
Pain referral. Periumbilical area and abdominal fullness
Abdominal pain. Midline abdominal aching that may mimic visceral pain from rectus trigger referral
Heartburn-like pain. Epigastric burning sensation from upper rectus trigger points mimicking gastric reflux
Lower sternum pain. Xiphoid process discomfort from upper rectus abdominis trigger point referral pattern
Pubic pain. Suprapubic aching from lower rectus abdominis trigger point referred pain pattern
Back pain. Horizontal band of low back pain referred from anterior rectus abdominis trigger points
Suprapubic pain mimicking bladder pathology. Lower rectus abdominis trigger points refer to the suprapubic region mimicking cystitis or interstitial cystitis
Lower abdominal cramping. Taut bands in the lower rectus create cramping pain in the lower abdominal wall
Urinary urgency (referred). Viscerosomatic convergence from lower abdominal trigger points creates perceived urinary urgency
Dysmenorrhea-like pain. Suprapubic referral mimics menstrual cramping through shared segmental innervation pathways
Inguinal region discomfort. Lateral referral from lower rectus extends to the inguinal region mimicking hernia or adductor pathology
Epigastric pain mimicking heartburn. Upper rectus trigger points near the xiphoid create epigastric pain mimicking gastroesophageal reflux
Bilateral mid-back ache. Posterior referral creates a horizontal band of aching across the bilateral mid-thoracic back
Substernal fullness sensation. Referral to the substernal area creates a sensation of pressure and fullness behind the sternum
Nausea (referred visceral). Viscerosomatic convergence from upper abdominal trigger points creates a referred nausea sensation
Upper abdominal wall tenderness. Taut bands in the upper rectus create palpable tenderness in the epigastric abdominal wall
Periumbilical cramping. Mid-belly rectus abdominis trigger points create cramping pain around the umbilical region
Abdominal bloating sensation. Trigger point-mediated abdominal wall tension creates a perceived bloating without actual distension
Mid-abdominal wall tenderness. Taut bands in the periumbilical rectus create localized abdominal wall tenderness on palpation
Functional abdominal pain. Somatic trigger point pain in the rectus mimics functional gastrointestinal disorders diagnostically
Sense of abdominal fullness without distension. Trigger point-mediated abdominal wall sensitivity creates fullness perception without visible distension
Sit-ups/crunches. Repetitive concentric loading of rectus abdominis during core exercises causes fiber overload
Coughing. Forceful repeated expiratory contractions strain rectus abdominis during prolonged cough episodes
Pregnancy. Sustained abdominal wall stretching during pregnancy overloads rectus abdominis eccentrically
Overexertion. Acute abdominal muscle overload during intense physical effort activates latent trigger points
Poor lifting technique. Excessive abdominal bracing during improper lifting overloads rectus abdominis fibers
Stress. Emotional tension causes chronic abdominal guarding and sustained rectus contraction
Excessive sit-ups or crunches. High-volume abdominal flexion exercises overload the lower rectus abdominis creating trigger points
Post-abdominal surgery adhesions. Surgical scarring restricts lower abdominal wall mobility creating compensatory trigger points
Chronic coughing. Repeated forceful coughing generates sustained lower rectus contraction and ischemic trigger points
Post-pregnancy diastasis recti. Abdominal wall separation alters rectus loading creating compensatory trigger points in remaining fibers
Heavy lifting with abdominal straining. Valsalva maneuver during heavy lifting generates extreme lower rectus abdominis contraction forces
Excessive crunches targeting upper abs. High-volume upper abdominal exercises overload the upper rectus abdominis fibers near the xiphoid
Chronic upper abdominal surgery adhesions. Upper abdominal surgical scarring restricts tissue mobility creating secondary trigger points
Prolonged forward flexed posture. Sustained trunk flexion shortens the upper rectus abdominis creating chronic ischemic trigger points
Chronic anxiety with abdominal bracing. Psychogenic abdominal guarding maintains chronic upper rectus contraction and trigger point formation
GERD-related chronic muscle guarding. Persistent epigastric discomfort from reflux creates secondary protective upper rectus guarding
Abdominal surgery with periumbilical incision. Surgical disruption at the periumbilical region creates scar tissue and persistent trigger points
Excessive core exercises. High-volume core training overloads the mid-rectus abdominis creating periumbilical trigger points
Chronic constipation with straining. Repeated Valsalva maneuver during straining generates sustained mid-abdominal wall contraction
Umbilical hernia repair adhesions. Post-hernia repair scarring restricts periumbilical tissue mobility creating compensatory trigger points
Prolonged seated posture compressing abdomen. Flexed sitting compresses the mid-abdominal wall creating sustained ischemia in periumbilical rectus
Lie face down and gently push your upper body up with your hands, keeping hips on the floor. Rise only to a comfortable level. This lengthens the rectus abdominis and can reduce the cramping sensation. Alternatively, stand and place your hands on your low back, gently leaning backward.
Apply a warm (not hot) heat pack over the painful area of the abdomen. Lie in a comfortable position with knees slightly bent to relax the abdominal wall. Breathe slowly and deeply, allowing the abdominal muscles to fully relax with each exhale.
Lie on your back with knees bent. Place one hand on your chest and one on your belly. Breathe in slowly through your nose, directing the breath into your belly (hand should rise). Exhale slowly through pursed lips. This relaxes the abdominal wall and reduces rectus abdominis tension.
Lie on your back with knees bent. Gently rock your pelvis back and forth — flatten your low back against the floor, then arch it slightly. This provides gentle mobilization and activation of the abdominal muscles without the strain of sit-ups or crunches.
Replace traditional sit-ups and crunches with planks, dead bugs, and bird-dogs, which strengthen the core without repetitively shortening the rectus abdominis. Avoid any exercise that reproduces or worsens the abdominal pain. Walk daily for 20-30 minutes as gentle core conditioning.
If abdominal pain persists beyond 2-3 weeks, consult a physician to rule out visceral causes first. Once GI, urinary, and gynecological conditions are excluded, a physiatrist can evaluate for abdominal wall trigger points using the Carnett test and provide targeted treatment.