TrP 1
TrP1
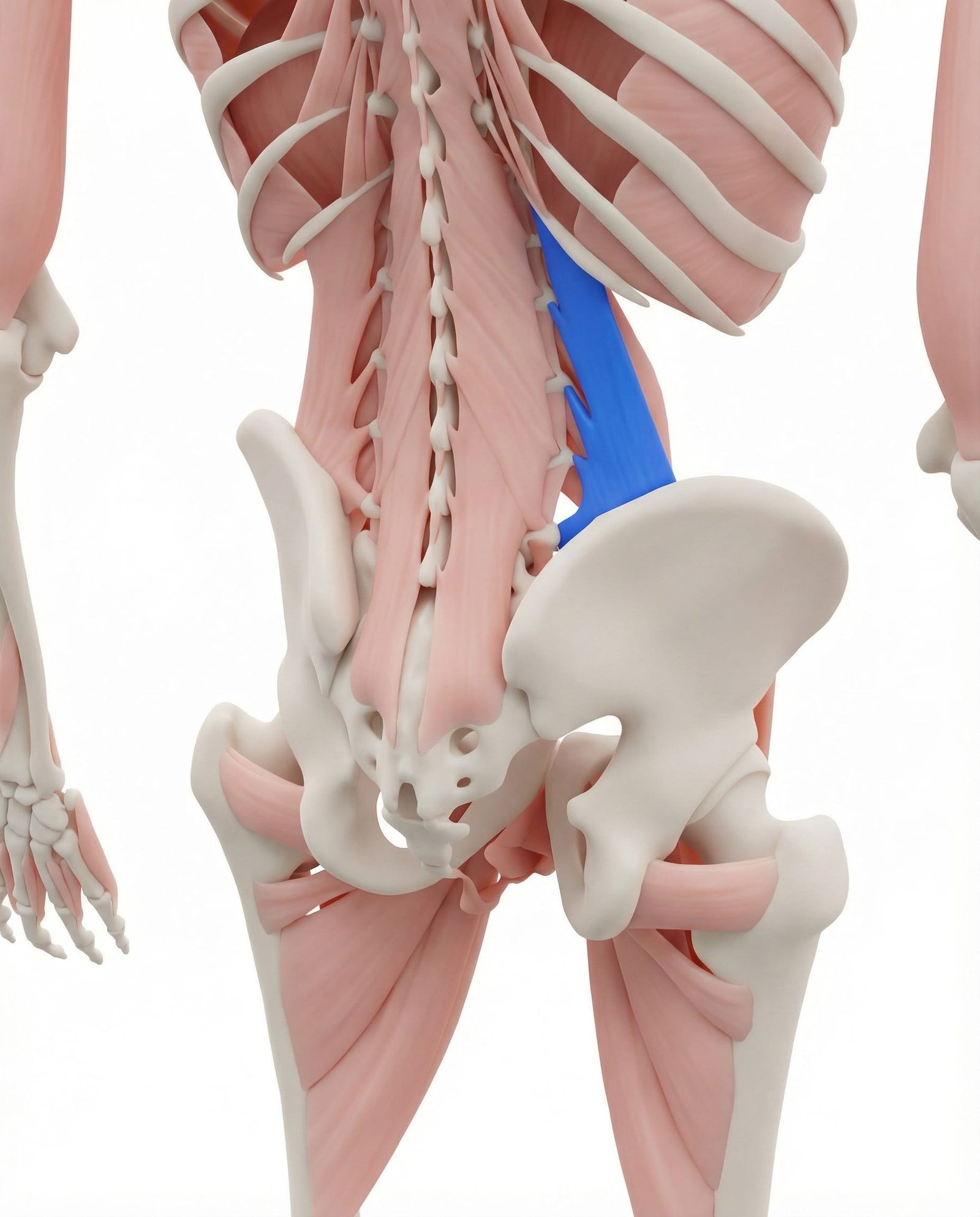
Location. Lower back, sides of spine
Pain referral. Lower back, hip, buttock
- Lower back
- Iliac crest
- Hip
- Buttock
- Groin
- Outer thigh
Deep unilateral lumbar aching along the iliac crest worsened by lateral trunk movements
Location. Lower back, sides of spine
Pain referral. Lower back, hip, buttock
Location. Lateral fibers of QL from iliac crest to 12th rib
Pain referral. Lateral hip and greater trochanter area
Location. Deep medial fibers of QL near lumbar transverse processes
Pain referral. SI joint and lower buttock
Location. Lower attachment of QL at iliac crest
Pain referral. Lower abdomen and groin
Lower back pain. Deep unilateral lumbar aching along the iliac crest worsened by lateral trunk movements
Hip pain. Referred ache over the greater trochanter and lateral hip from QL trigger points
Difficulty standing straight. Protective lateral trunk shift from QL spasm preventing full upright posture
Pain when coughing/sneezing. Sharp lumbar spike during forced expiration as intra-abdominal pressure loads the QL
Stiffness in morning. Sustained shortened QL position during sleep causes morning lumbar rigidity on waking
Lateral hip pain mimicking bursitis. Superficial QL trigger point refers pain to greater trochanter mimicking trochanteric bursitis
Pain along iliac crest. Trigger point at QL iliac crest attachment creates localized periosteal pain along crest
Difficulty lying on affected side. Side-lying compresses lateral QL fibers against iliac crest aggravating trigger point
Lower flank pain. Superficial QL trigger point produces lateral trunk pain in lower flank region
Pain with side bending away. Contralateral side bending stretches taut QL fibers across the active trigger point
SI joint pain. Deep QL trigger point refers medially to sacroiliac region mimicking SI joint dysfunction pattern
Deep lower buttock ache. Referred pain from deep QL fibers descends to upper medial gluteal and lower buttock area
Pain transitioning from sit to stand. Sit-to-stand requires lumbar extension loading deep QL fibers at transverse process attachments
Lower back stiffness. Taut deep QL bands restrict segmental lumbar mobility creating lower back rigidity sensation
Difficulty finding comfortable position. Deep QL trigger point is aggravated by multiple positions creating persistent positional discomfort
Lower abdominal pain. QL iliac attachment trigger point refers anteriorly to lower abdominal wall mimicking visceral pain
Groin ache. Referred pain from QL iliac crest travels anteroinferiorly to inguinal and groin region
Pain mimicking inguinal hernia. Inguinal referred pain from QL trigger point creates false impression of herniation
Discomfort at hip bone in front. Referred pain to ASIS region from QL iliac crest trigger point periosteal irritation
Pain with hip flexion. Hip flexion alters pelvic mechanics stressing QL iliac attachment and active trigger point
Lifting with poor form. Asymmetric lifting loads QL eccentrically as it attempts to stabilize the lumbar spine
Prolonged sitting. Sustained seated posture shortens QL and reduces blood flow causing ischemic trigger points
Uneven pelvis. Pelvic obliquity forces one-sided QL overactivation to maintain spinal vertical alignment
Leg length difference. Structural or functional limb asymmetry chronically overloads QL on the longer-leg side
Weak core. Insufficient core stabilization forces QL to compensate as primary lateral trunk stabilizer
Pregnancy. Anterior weight shift and lordotic increase overload QL for trunk extension support
Repetitive bending. Continuous lateral or forward bending fatigues QL beyond its recovery capacity
Leg length discrepancy. Unequal leg lengths create chronic lateral pelvic tilt overloading QL on shorter side
Scoliosis. Spinal curvature creates asymmetric QL loading with trigger points on convex side
Lifting heavy objects to one side. Asymmetric lifting requires unilateral QL lateral stabilization exceeding fiber capacity
Sleeping on a sagging mattress. Mattress sag creates lateral trunk flexion sustaining QL in awkward shortened position
Repetitive side-bending activities. Repeated lateral flexion fatigues superficial QL fibers from iliac crest to twelfth rib
Carrying child on one hip. Asymmetric load carrying demands sustained unilateral QL contraction for pelvic stabilization
Heavy lifting with poor mechanics. Improper lifting technique overloads deep QL fibers that stabilize lumbar transverse processes
Prolonged sitting with poor lumbar support. Seated posture without lumbar support increases deep QL demand for segmental stabilization
Gardening and yard work. Prolonged trunk flexion and rotation during gardening overloads deep QL stabilizing fibers
Weak deep core muscles. Insufficient transversus abdominis and multifidus strength forces deep QL to compensate
Post-lumbar surgery deconditioning. Surgical deconditioning weakens deep stabilizers overloading deep QL during recovery activities
Chronic constipation straining. Repeated Valsalva straining increases intra-abdominal pressure stressing deep QL attachments
Chronic coughing. Repeated forceful coughing increases intra-abdominal pressure stressing QL iliac crest attachment
Heavy deadlifting. Maximal lumbar extension loading during deadlift overloads QL at iliac crest insertion
Straining with constipation. Valsalva straining with bearing down stresses QL lower attachment against iliac crest
Prolonged standing. Static standing demands sustained QL iliac attachment loading for lateral pelvic stabilization
Repetitive bending and lifting. Cyclic trunk flexion-extension repeatedly loads QL iliac crest attachment beyond recovery
Pregnancy and postpartum. Pregnancy weight gain and postpartum recovery overload QL iliac attachment through altered mechanics
Lie on your non-painful side on the floor or a firm bed. Place a thick pillow or rolled-up blanket under your waist so that your waist is propped up and the painful side is on top, stretched open. Let your top arm reach overhead to lengthen the stretch further. Allow gravity to gently open and stretch the QL on the upper side. Breathe deeply into the stretch and let the muscle gradually release.
Lie on your back with knees bent. Place a tennis ball on the floor beside your spine at waist level, in the thick muscle between the bottom rib and the top of the pelvis. Slowly shift your weight onto the ball and gently roll up and down and side to side over the tender area. Pause on especially sore spots for 20-30 seconds. Use your feet to control how much body weight presses onto the ball.
For cat-cow: Start on hands and knees. Inhale as you arch your back, letting your belly drop toward the floor (cow). Exhale as you round your back upward, tucking your chin and pelvis (cat). Move slowly through 10 cycles. For child's pose with side reach: From hands and knees, sit back onto your heels with arms extended forward. Walk both hands to one side until you feel a stretch along the opposite waist and lower back. Hold for 30 seconds, then switch sides.
Lie on your side with your elbow directly under your shoulder and knees bent at 90 degrees for the modified version. Lift your hips off the floor so your body forms a straight line from head to knees. Hold this position while keeping your core engaged. For the full version, extend your legs and support yourself on your elbow and the side of your bottom foot. Start with the modified version and progress as strength allows.
Stand with your feet shoulder-width apart. Raise the arm on the painful side overhead and slowly bend your trunk to the opposite side, reaching your raised hand over your head. You should feel a stretch along the waist and lower back on the raised-arm side. Keep both feet firmly planted and avoid rotating your trunk. Use the opposite hand on your hip for support.
Avoid prolonged sitting by standing up and moving every 30-45 minutes. Use a chair with good lumbar support that keeps your hips and knees at 90-degree angles. When standing, distribute your weight evenly between both feet and avoid leaning to one side or hip-hiking. When lifting, bend at the knees and hips rather than the waist, and keep the load close to your body. If you have a leg length difference, consider a heel lift after professional assessment.
If deep lower back and flank pain persists despite 4-6 weeks of stretching, strengthening, and ergonomic changes, seek evaluation from a healthcare provider. They can assess for sacroiliac joint dysfunction, leg length discrepancy, pelvic obliquity, or lumbar disc issues that may be contributing to QL overload. A physical therapist can provide targeted manual therapy including QL release techniques that are difficult to perform on yourself.