TrP 1
TrP1
Location. Deep hip, lateral rotator
Pain referral. Deep buttock, hip
- Deep buttock
- Hip
- Posterior thigh
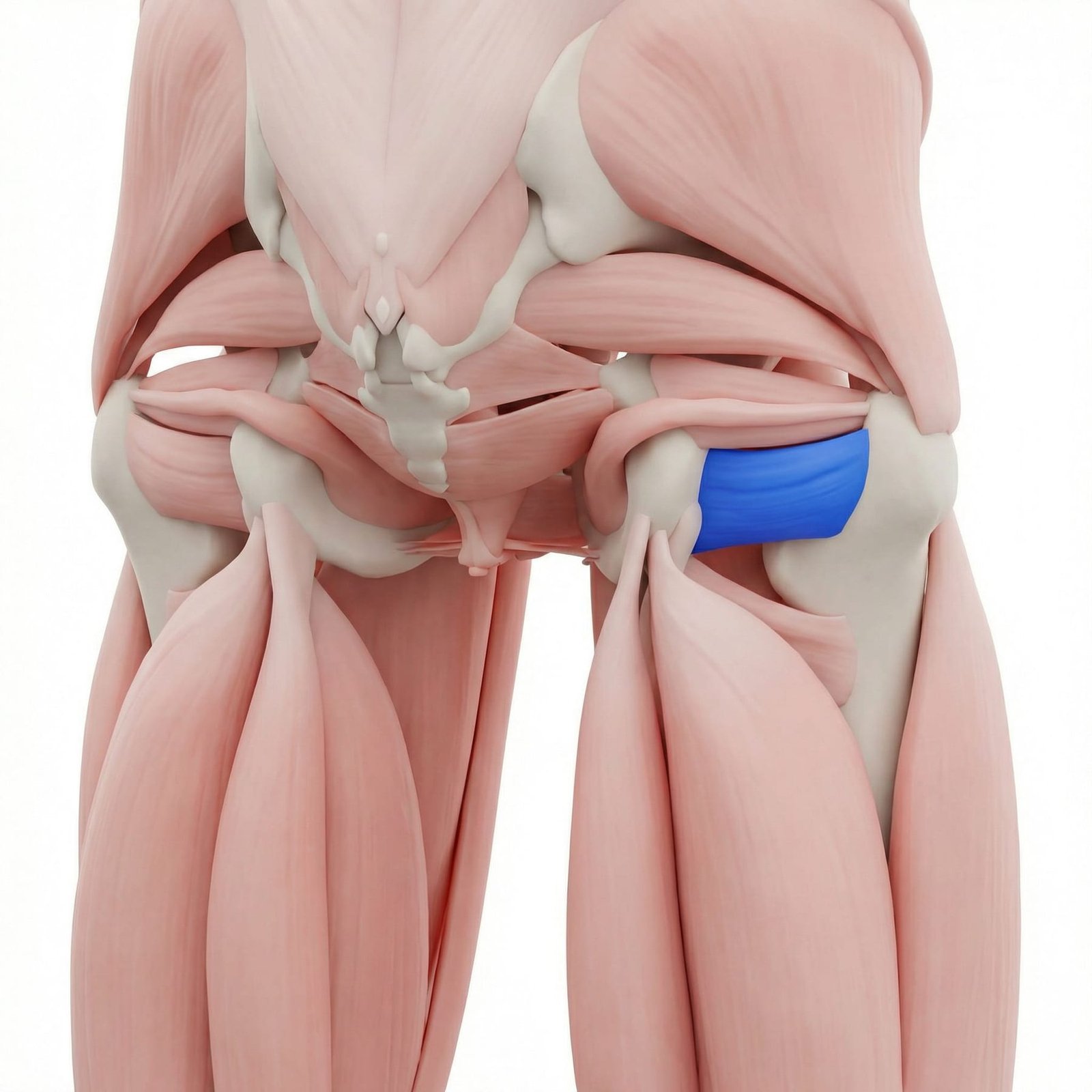
Deep gluteal pain from quadratus femoris trigger points between ischium and femur
Location. Deep hip, lateral rotator
Pain referral. Deep buttock, hip
Location. Near greater trochanter attachment
Pain referral. Deep posterior hip and lateral hip
Deep hip pain. Deep gluteal pain from quadratus femoris trigger points between ischium and femur
Buttock pain. Inferior gluteal aching from deep external rotator trigger point referral pattern
Lateral rotation pain. Pain during hip external rotation loading compromised quadratus femoris trigger point fibers
Deep buttock ache. Deep posterior hip ache from quadratus femoris trigger point between ischium and greater trochanter
Pain with hip rotation. Both internal and external rotation stress quadratus femoris aggravating active trigger points
Posterior hip tenderness. Deep posterior hip palpation reproduces quadratus femoris trigger point tenderness and referral
Difficulty sitting cross-legged. Cross-legged position requires hip external rotation that loads sensitized quadratus femoris
Pain radiating down posterior thigh (mild). Mild posterior thigh referral from quadratus femoris trigger point overlapping sciatic nerve zone
Running. Repetitive hip rotation during running gait cumulatively overloads quadratus femoris stabilizer
Hip rotation. Forceful or sustained external rotation overloads quadratus femoris short rotator fibers
Sitting. Prolonged sitting compresses deep hip rotators between pelvis and chair causing ischemia
Sports. Activities requiring hip rotation overload deep lateral rotator muscle group chronically
Hip external rotation overuse. Repetitive external rotation activities overload quadratus femoris as a primary external rotator
Ballet (turnout positions). Sustained turnout posture maximally loads quadratus femoris through chronic external rotation demand
Martial arts kicking. High-velocity hip rotation during kicks creates eccentric quadratus femoris overload repetitively
Post-hip replacement compensation. Altered hip mechanics after replacement shifts load to deep rotators including quadratus femoris
Chronic sitting with crossed legs. Sustained external rotation during cross-legged sitting shortens quadratus femoris chronically
Sit on a firm surface and place a tennis ball directly under the lower buttock near the sit bone on the affected side. Slowly shift your weight onto the ball, targeting the tender area between the sit bone and the outer hip. Hold sustained pressure on sore spots for 20-30 seconds. Adjust the ball position to cover the entire area around the ischial tuberosity.
Sit on a chair with knees bent 90 degrees and feet flat on the floor wider than hip-width apart. Keeping the affected knee still, swing the foot outward to internally rotate the hip. You should feel a stretch deep in the buttock near the sit bone. Hold for 20-30 seconds and relax. Use your hand on the knee to gently guide the stretch if needed.
Lie on your side with hips and knees bent to about 60 degrees. Keeping feet together, lift the top knee upward while keeping your pelvis stable. Pause at the top for 2-3 seconds, then lower slowly. To increase difficulty, add a resistance band around both knees. Focus on slow, controlled movements.
Lie on your back with knees bent and feet flat on the floor hip-width apart. With a resistance band around your knees, press your knees slightly outward to engage the deep hip rotators, then lift your hips toward the ceiling. Hold the top position for 3-5 seconds while maintaining the outward knee pressure, then lower slowly. This strengthens both glutes and deep rotators simultaneously.
Use a well-padded seat cushion or folded towel to reduce direct pressure on the sit bones during prolonged sitting. Avoid hard wooden or metal chairs when possible. Stand up and walk for 2-3 minutes every 30 minutes. When sitting, shift your weight periodically from one side to the other to vary pressure distribution.
If sit bone pain persists beyond 4 weeks of self-care, consult a physiotherapist or sports medicine specialist. They can differentiate quadratus femoris trigger points from hamstring tendinopathy, ischial bursitis, sciatic nerve irritation, or stress fractures through clinical examination and imaging. Targeted deep tissue work and dry needling can effectively treat this hard-to-reach muscle.