TrP 1
TrP1
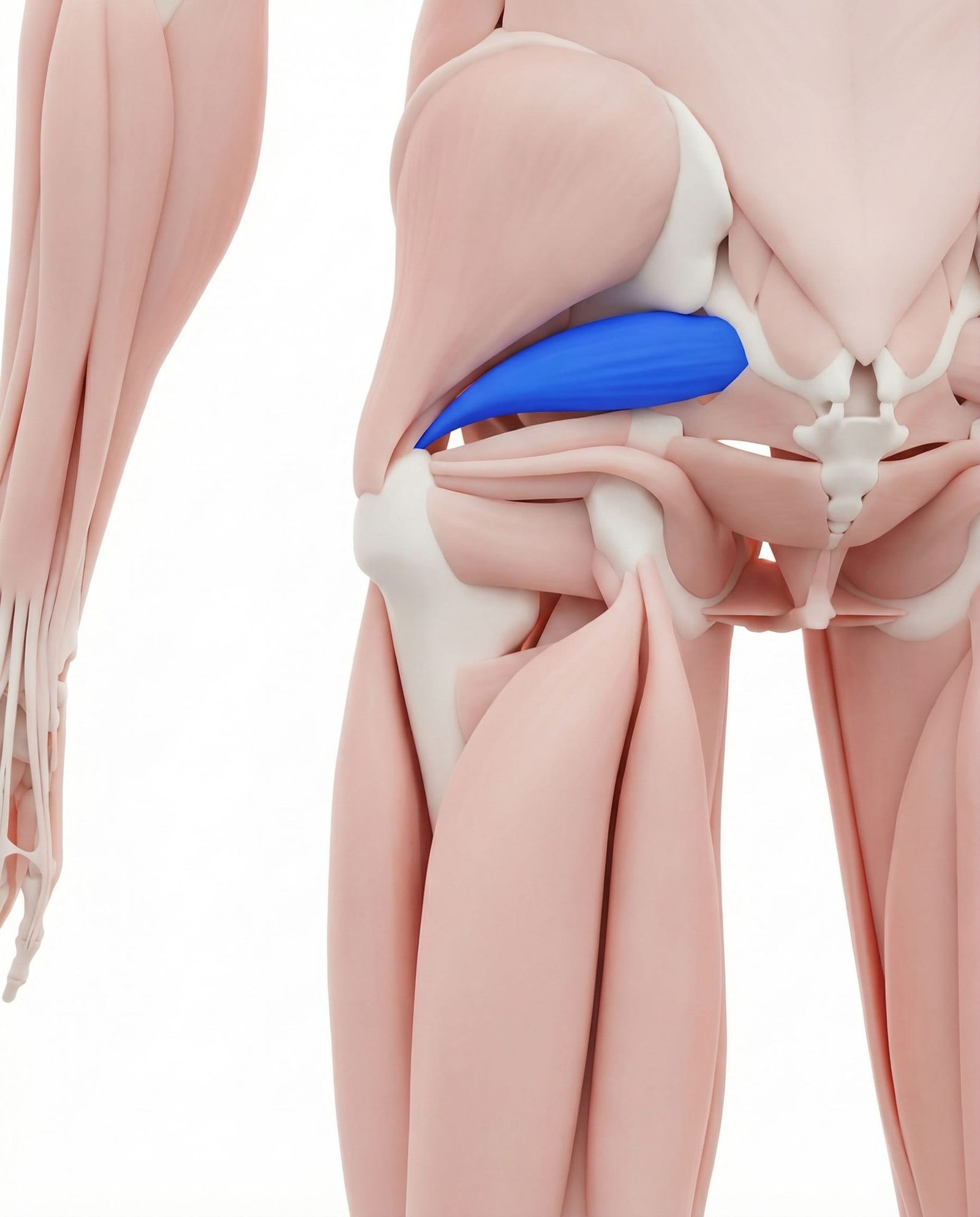
Location. Deep buttock, near sciatic nerve
Pain referral. Buttock, back of thigh, calf
- Buttock
- Back of thigh
- Calf
- Lower back
- Hip
Deep central buttock aching from piriformis trigger points near the sciatic notch
Location. Deep buttock, near sciatic nerve
Pain referral. Buttock, back of thigh, calf
Location. Deep buttock, near sciatic nerve
Pain referral. Deep buttock, posterior leg
Location. Near sacral attachment of piriformis
Pain referral. Posterior hip joint and lower sacroiliac area
Location. Near greater trochanter insertion of piriformis
Pain referral. Posterior thigh mimicking sciatica
Buttock pain. Deep central buttock aching from piriformis trigger points near the sciatic notch
Sciatica-like pain. Radiating posterior leg pain from piriformis compression or irritation of sciatic nerve
Sitting pain. Increased buttock aching when seated from direct compression of piriformis trigger points
Hip pain. Deep posterior hip aching from piriformis tension affecting the hip joint capsule
Leg numbness/tingling. Paresthesia in posterior leg from piriformis mechanical compression of the sciatic nerve
Deep buttock pain. Intense deep gluteal aching from piriformis trigger point near sciatic nerve proximity
Sciatica-like symptoms. Radiating posterior leg pain from piriformis compression or irritation of the sciatic nerve
Posterior hip pain. Sacral piriformis trigger point refers deep aching to posterior hip joint capsule region
SI joint area pain. Trigger point proximity to sacrum creates localized pain mimicking sacroiliac joint dysfunction
Deep buttock ache. Piriformis trigger point near sacral origin produces deep poorly localized gluteal aching
Pain sitting on affected side. Seated compression of ischial region loads piriformis sacral trigger point against pelvic bone
Hip stiffness on internal rotation. Taut piriformis band resists hip internal rotation creating palpable end-range restriction
Sciatica-like pain down posterior leg. Piriformis insertion trigger point compresses or irritates sciatic nerve creating pseudosciatica
Posterior thigh burning. Neural irritation from piriformis trigger point produces burning dysesthesia in posterior thigh
Tingling in posterior thigh. Sciatic nerve compression at piriformis level creates posterior thigh paresthesia and tingling
Sitting intolerance. Seated hip flexion compresses piriformis against sciatic nerve increasing posterior leg symptoms
Pain that increases with hip flexion and internal rotation. Combined flexion and internal rotation maximally stretches piriformis compressing sciatic nerve
Prolonged sitting. Sustained compression of piriformis between ischial tuberosity and seating surface creates ischemia
Running. Repetitive hip external rotation demand during running stride fatigues piriformis each cycle
Climbing. Sustained hip rotation and extension during climbing overloads the piriformis muscle
Falls on buttock. Direct trauma to buttock from falls acutely damages piriformis fibers near sciatic nerve
Leg length discrepancy. Pelvic asymmetry from limb length difference chronically overloads piriformis on one side
Pregnancy. Increased pelvic width and altered gait mechanics during pregnancy stress the piriformis
Falls. Direct impact on buttock traumatizes piriformis muscle fibers creating acute trigger point formation
Leg length difference. Pelvic obliquity from leg length discrepancy creates asymmetric piriformis loading and shortening
Prolonged sitting on wallet. Wallet in back pocket elevates one ischium creating asymmetric piriformis compression and ischemia
Driving long distances. Sustained hip flexion with vibration during driving fatigues piriformis in shortened position
Falls onto buttock. Direct impact trauma to buttock damages piriformis fibers near sacral origin creating trigger points
Chronic low back dysfunction. Lumbar pathology alters pelvic mechanics creating compensatory piriformis overactivation at sacrum
Asymmetric pelvic alignment. Pelvic obliquity creates uneven piriformis loading with sacral trigger point on compressed side
Running on hard surfaces. Impact loading during running transmits force through piriformis at trochanteric insertion
Hip trauma or falls. Direct buttock trauma injures piriformis near insertion creating post-traumatic trigger points
Post-hip surgery compensation. Altered hip biomechanics after surgery overloads piriformis as compensatory external rotator
Cycling with improper seat height. Incorrect saddle height alters hip mechanics creating abnormal piriformis loading during pedaling
Lie on your back with both knees bent and feet flat on the floor. Cross the ankle of the affected side over the opposite knee, creating a figure-4 shape. Reach through and grasp the thigh of the bottom leg, then gently pull it toward your chest until you feel a deep stretch in the buttock of the crossed leg. Keep your head and shoulders relaxed on the floor throughout.
Sit on a firm surface such as the floor or a wooden chair. Place a tennis ball directly under the deep center of your buttock on the affected side, roughly halfway between the sit bone and the outer hip. Lean your body weight onto the ball and slowly roll around, pausing on any particularly tender spots. You can also do this lying on your back with knees bent for more control over pressure.
Sit upright in a firm chair with both feet flat on the floor. Cross the affected leg so the ankle rests on the opposite knee. Keeping your back straight, gently lean forward from the hips until you feel a deep stretch in the buttock. You can use your hand to gently press the crossed knee downward for a deeper stretch. Hold the position while breathing deeply.
Lie on your back with both knees bent and feet flat on the floor, wider than hip-width apart. Let both knees drop inward toward the midline so the inner knees move toward each other. You should feel a gentle stretch deep in both buttocks. Alternatively, sit on the floor with knees bent, feet wide, and let one knee drop inward at a time. Hold each position and breathe deeply.
Lie on your back with knees bent and feet flat on the floor, hip-width apart. Squeeze your glutes and lift your hips off the floor until your body forms a straight line from shoulders to knees. Hold the top position for 3-5 seconds, focusing on squeezing the large gluteal muscles rather than the deep buttock. Lower slowly and repeat. This strengthens the gluteus maximus so the piriformis does not have to compensate.
Remove your wallet, phone, or any objects from your back pocket before sitting, as these create uneven pressure directly over the piriformis. Set a timer to stand and stretch every 30 minutes during sedentary work. When driving long distances, plan stops every 45-60 minutes to get out and do a quick piriformis stretch. Avoid crossing your legs when seated, as this shortens and compresses the piriformis.
If you experience numbness, tingling, or pain radiating below the knee that does not improve with 4-6 weeks of stretching and self-care, seek evaluation from a healthcare provider. They can perform specific tests to differentiate piriformis syndrome from lumbar disc herniation or other spinal causes of sciatica. Imaging such as MRI may be needed to rule out disc pathology.
Lie on your back with both knees bent and feet flat on the floor. Cross the affected ankle over the opposite knee to form a figure-four shape. Reach both hands behind the uncrossed thigh and gently pull it toward your chest until you feel a deep stretch in the buttock of the crossed leg. Keep your head and shoulders relaxed on the floor. Hold the stretch without bouncing.
Sit on a firm surface and place a tennis ball under the affected buttock, positioning it between the sacrum and the greater trochanter. Lean your weight onto the ball and slowly roll in small circles to locate the most tender spot. Once found, hold sustained pressure on that point for 30-60 seconds until the tenderness begins to diminish. Shift slightly to address adjacent tender areas. Use a softer ball if the pressure is too intense.
Lie on your side with hips and knees bent to approximately 45 degrees and feet together. Keeping your feet in contact, slowly lift the top knee as far as comfortable without rotating your pelvis backward. Hold at the top for 2 seconds, then lower slowly. Focus on feeling the contraction deep in the buttock. Add a resistance band around the knees once the exercise feels easy.
Lie face down with your forehead resting on your hands. Bend the affected knee to 90 degrees, then lift the knee slightly off the floor while rotating the foot inward (this externally rotates the hip). Hold for 3 seconds at the top, then slowly lower. Keep your pelvis flat against the floor throughout to isolate the deep hip rotators. Perform the movement slowly and with control.
Set a timer to stand and move every 30-45 minutes during desk work or driving. During breaks, perform 30 seconds of standing hip circles or gentle figure-four stretches. Use a seat cushion with a coccyx cutout to reduce direct pressure on the piriformis while seated. When driving long distances, plan stops every hour to walk for 2-3 minutes. Avoid crossing the legs while seated as this increases piriformis tension.
If deep buttock pain with radiating leg symptoms persists beyond 4 weeks of self-treatment, or if you develop progressive weakness in the foot or leg, consult an orthopedic specialist or neurologist. The clinician can perform nerve conduction studies, MRI of the lumbar spine and pelvis, and specific provocative tests to distinguish piriformis syndrome from lumbar disc herniation or sacroiliac joint dysfunction. Targeted treatments such as guided injection, dry needling, or manual therapy may be recommended.