TrP 1
TrP1
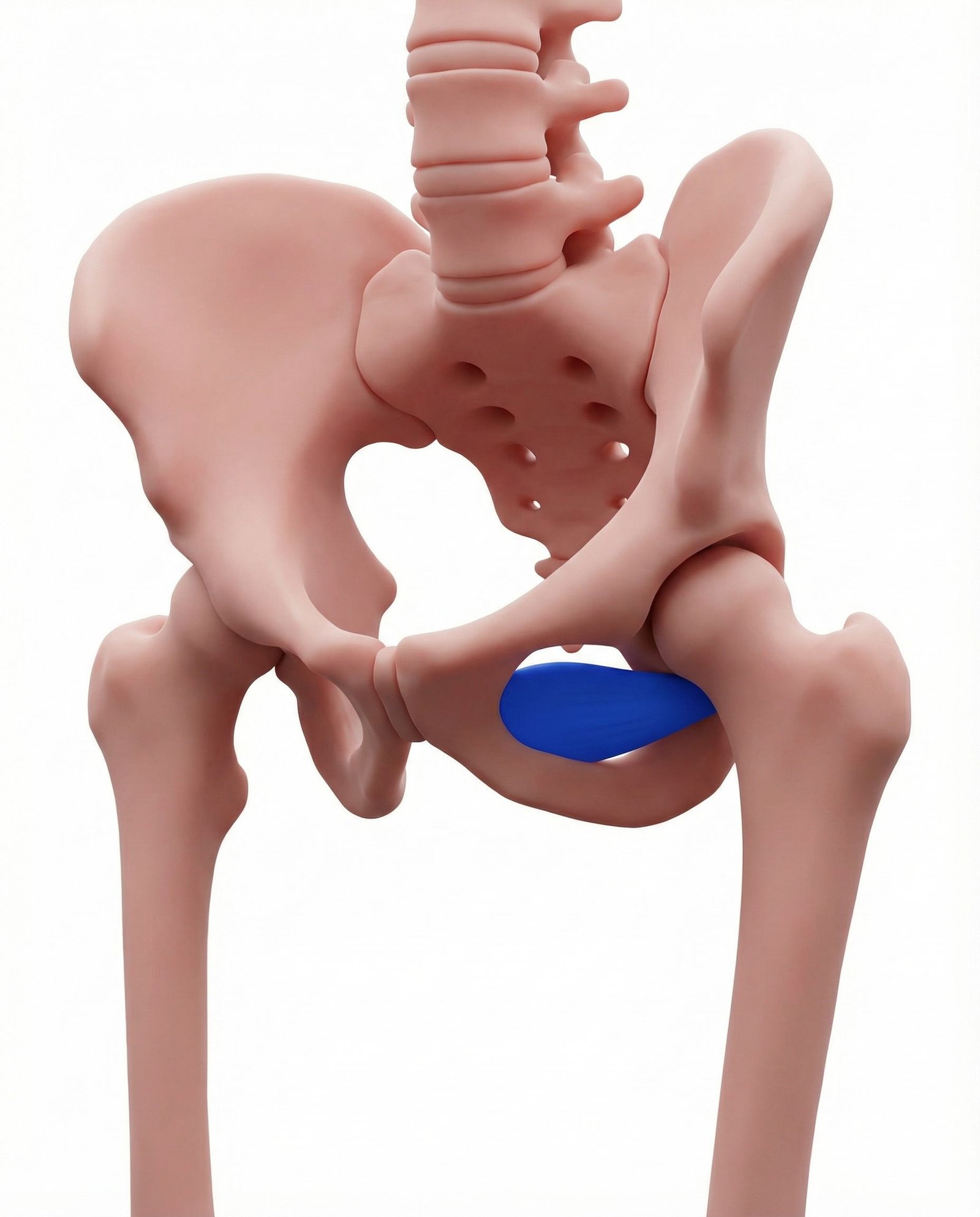
Location. Deep hip, anterior
Pain referral. Groin, hip, anterior thigh
- Groin
- Hip
- Anterior thigh
Deep inguinal aching from obturator externus trigger points near obturator foramen region
Location. Deep hip, anterior
Pain referral. Groin, hip, anterior thigh
Location. Near trochanteric fossa insertion
Pain referral. Deep groin and medial thigh
Groin pain. Deep inguinal aching from obturator externus trigger points near obturator foramen region
Hip pain. Anterior hip joint pain from obturator externus trigger point referral to hip capsule area
Thigh discomfort. Anterior thigh aching from obturator externus distal trigger point referral pattern
Deep groin pain. Deep groin ache from obturator externus trigger point referral through obturator foramen region
Medial thigh ache. Referred medial proximal thigh pain from obturator externus trigger point near trochanteric fossa
Pain with hip adduction. Hip adduction loads obturator externus in its secondary role aggravating active trigger points
Deep hip joint sensation. Obturator externus trigger point referral mimics intra-articular hip pathology due to deep location
Difficulty with wide-stance activities. Wide stance positions stretch obturator externus aggravating trigger points near trochanteric insertion
Running. Repetitive hip rotation during running gait cumulatively overloads obturator externus fibers
Hip rotation. Sustained or forceful hip external rotation overloads obturator externus muscle directly
Sports. Activities requiring hip rotation and adduction control overload obturator externus chronically
Overuse. Exceeding deep hip rotator recovery capacity creates persistent obturator externus dysfunction
Adductor overuse activities. Activities requiring forceful adduction co-activate obturator externus creating secondary overload
Ice skating or skiing. Lateral leg movements in skating and skiing cyclically load obturator externus through rotation
Post-hip surgery guarding. Protective deep rotator guarding after hip surgery creates sustained obturator externus contraction
Chronic adductor strains. Repeated adductor injuries create compensatory obturator externus overload during recovery phases
Horseback riding. Sustained adduction and external rotation during riding overloads obturator externus chronically
Lie on your back with the affected knee bent and foot flat on the floor. Let the knee fall outward to expose the inner thigh. Using your thumbs, apply firm sustained pressure to the soft tissue in the upper inner groin crease, approximately 3-5 cm lateral to the pubic bone. Press slowly and deeply toward the obturator foramen area. When you find a particularly tender spot, hold steady pressure for 20-30 seconds. Work systematically across the upper inner groin region.
Sit on the floor with the soles of your feet together and knees out to the sides in a butterfly position. Gently press the knees toward the floor using your elbows while keeping your back straight. Hold for 30 seconds. To increase the stretch on the obturator externus, lean your upper body slightly forward from the hips while maintaining a straight spine. You should feel a deep stretch in the inner groin and upper inner thigh.
Lie on your side with the affected leg on the bottom. Bend the top leg and place the foot flat on the floor in front of the bottom knee for stability. Keeping the bottom leg straight, lift it upward toward the ceiling, then slowly rotate the hip so the toes point slightly upward at the top of the movement. Hold for 3 seconds, then lower slowly. This engages the obturator externus through combined adduction and rotation. Progress by adding a light ankle weight.
Sit on the edge of a chair with feet flat on the floor, hip-width apart. Place a resistance band looped around both knees. Keeping your feet planted, slowly press both knees outward against the band resistance, externally rotating the hips. Hold for 5 seconds, then slowly return. Next, with the band still on, try to bring your knees together against the band for 5 seconds. This alternating rotation pattern strengthens the obturator externus and its antagonists for balanced hip function.
Avoid prolonged sitting with legs crossed, as this places the obturator externus in a shortened, compressed position. During sports, warm up the hip rotators with gentle leg swings and circles before vigorous activity. If you sit at a desk, keep your feet flat on the floor with hips and knees at approximately 90 degrees. Avoid sudden pivoting or twisting movements on a planted foot during recreational activities until the trigger point has resolved.
If deep groin or anterior hip pain persists beyond 4 weeks despite self-care, consult a physiotherapist, sports medicine specialist, or orthopedic surgeon. The obturator externus is a deep, difficult-to-access muscle that may require professional manual therapy, dry needling under ultrasound guidance, or specific rehabilitation protocols. A specialist can rule out hip labral tears, femoral acetabular impingement, sports hernia, or adductor tendinopathy that may present similarly.