TrP 1
TrP1
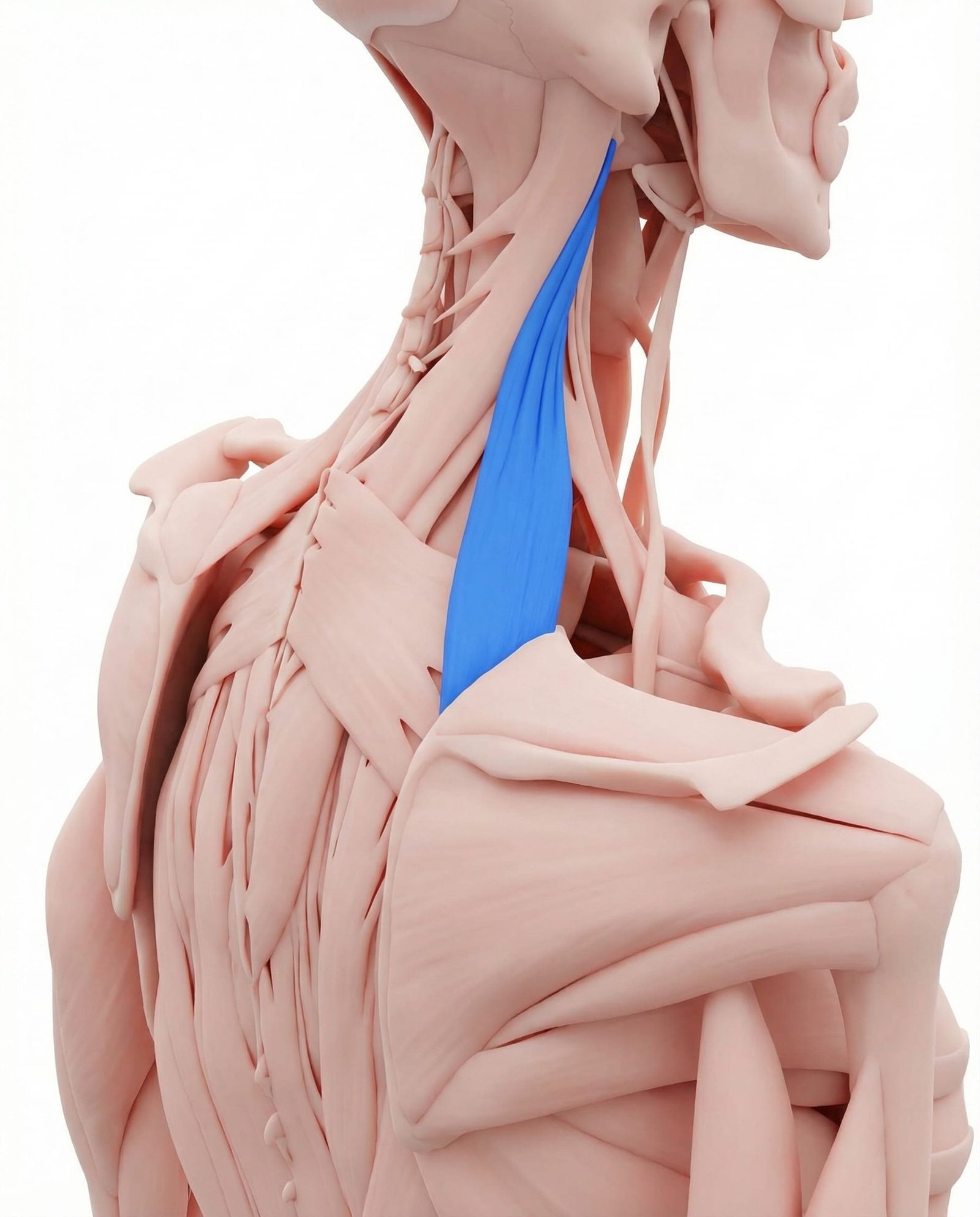
Location. Neck to shoulder blade (medial border)
Pain referral. Neck and upper shoulder
- Neck angle
- Shoulder blade inner edge
- Back of shoulder
Persistent aching at the neck-shoulder angle even without movement or loading
Location. Neck to shoulder blade (medial border)
Pain referral. Neck and upper shoulder
Location. Mid-belly of levator scapulae at C3-C4 level
Pain referral. Posterior shoulder and scapula
Location. Near superior angle of scapula at levator scapulae insertion
Pain referral. Medial scapular border with intense focal pain
Neck pain at rest. Persistent aching at the neck-shoulder angle even without movement or loading
Difficulty turning head. Restricted cervical rotation especially toward the affected side from taut bands
Shoulder blade pain. Referred ache along the superior medial scapular border near the attachment site
Stiff neck. Morning cervical rigidity from sustained shortened position during sleep
Posterior shoulder ache. Levator scapulae TrP2 refers aching to posterior shoulder via scapular elevation pathway
Restricted neck rotation. Taut levator scapulae band mechanically limits cervical rotation to the affected side
Pain at angle of neck and shoulder. Trigger point at cervicoscapular junction creates localized pain at neck-shoulder angle
Stiff neck on affected side. Shortened levator scapulae fibers restrict ipsilateral cervical lateral flexion and rotation
Difficulty looking over shoulder. Combined cervical rotation and extension limited by taut levator scapulae restricting movement
Intense focal pain at inner shoulder blade. Levator scapulae insertion trigger point creates exquisitely tender point at superior scapular angle
Restricted neck rotation to affected side. Taut levator scapulae at insertion limits ipsilateral cervical rotation mechanically
Deep scapular ache. Trigger point at scapular attachment produces deep periosteal aching at bone-tendon interface
Pain with deep inspiration. Rib cage expansion during deep breath moves scapula stressing irritated levator insertion
Shoulder blade grinding sensation. Taut levator scapulae alters scapulothoracic mechanics creating crepitus at scapular angle
Looking down at phone. Sustained cervical flexion overloads levator scapulae as it resists head weight
Computer work. Forward head posture at a desk chronically shortens and overloads levator scapulae
Stress. Emotional tension causes habitual shoulder hiking and sustained levator scapulae contraction
Sleeping with poor pillow. Improper cervical support during sleep sustains awkward neck position straining muscle
Reading in bed. Prolonged neck flexion while propped up places sustained load on levator scapulae
Carrying heavy bags. Shoulder strap weight forces reactive levator scapulae contraction to stabilize scapula
Sleeping with poor pillow support. Inadequate cervical support during sleep sustains levator scapulae in awkward lengthened position
Carrying heavy bag on one shoulder. Unilateral shoulder depression forces ipsilateral levator scapulae eccentric overload
Prolonged phone cradling. Sustained lateral cervical flexion to hold phone shortens ipsilateral levator scapulae
Cold drafts on neck. Cold exposure triggers protective cervical muscle guarding with sustained levator scapulae contraction
Stress-related shoulder hiking. Habitual stress response elevates scapulae via sustained levator scapulae activation
Sustained neck rotation (e.g., side monitor). Chronic unilateral neck rotation to view side monitor overloads levator scapulae asymmetrically
Chronic forward head posture. Sustained anterior head position eccentrically overloads levator scapulae at scapular insertion
Repetitive overhead reaching. Repeated scapular upward rotation stretches levator scapulae insertion beyond comfortable range
Backpack carrying. Downward scapular traction from backpack weight eccentrically loads levator scapulae insertion
Side sleeping with poor arm support. Unsupported arm weight during side sleeping depresses scapula straining levator insertion
Emotional stress. Chronic stress-driven scapular elevation creates sustained tension at levator scapulae insertion
Prolonged reading with neck flexion. Sustained neck flexion during reading eccentrically loads levator scapulae at scapular attachment
Stand with your back against a wall. Place a tennis ball at the angle where your neck meets the top of your shoulder blade — the most tender area. Lean into the ball with moderate pressure and slowly tilt your head away from the ball to increase the stretch. Hold sustained pressure on tender spots for 30-60 seconds until you feel a softening or release.
Apply a warm, damp towel or microwaveable heat pack to the side and back of the neck, extending down to the upper shoulder blade area. Lie on your back with the heat pack underneath you for best coverage. Keep the heat comfortably warm and relax your shoulders completely.
Sit upright. Turn your head 45 degrees to the right, then tilt your chin down as if looking into your right armpit. Place your right hand on the back of your head and apply gentle downward pressure — just enough to deepen the stretch, not force it. You should feel a stretch at the back-left angle of your neck. Hold for 30 seconds, then switch sides.
Sit or stand with arms at your sides. Squeeze your shoulder blades together as if trying to hold a pencil between them. Hold for 5 seconds, then relax. Keep your shoulders down — do not shrug while squeezing. Focus on engaging the muscles between your shoulder blades rather than your upper trapezius.
Sit upright with shoulders relaxed. Slowly turn your head to the right as far as comfortable, hold for 10 seconds. Return to center. Slowly turn to the left, hold for 10 seconds. Repeat 5 times each direction. Move slowly and smoothly — never jerk or force the rotation. If one side is more restricted, spend extra time with gentle holds in that direction.
If you sleep on your side, use a pillow thick enough to keep your head level with your spine — the ear should be directly above the shoulder. If you sleep on your back, use a thinner pillow that supports the natural cervical curve without pushing the head forward. Avoid sleeping on your stomach, which forces extreme cervical rotation. Consider a contoured cervical pillow designed for neck support.
If the stiff neck does not significantly improve within 2-3 weeks of consistent stretching and self-care, consult a physiatrist or pain specialist. They can assess whether trigger point treatment, manual therapy, or further evaluation for cervical spine pathology is needed. Mention specific limitations such as difficulty checking blind spots while driving or inability to turn the head in one direction.