TrP 1
TrP1
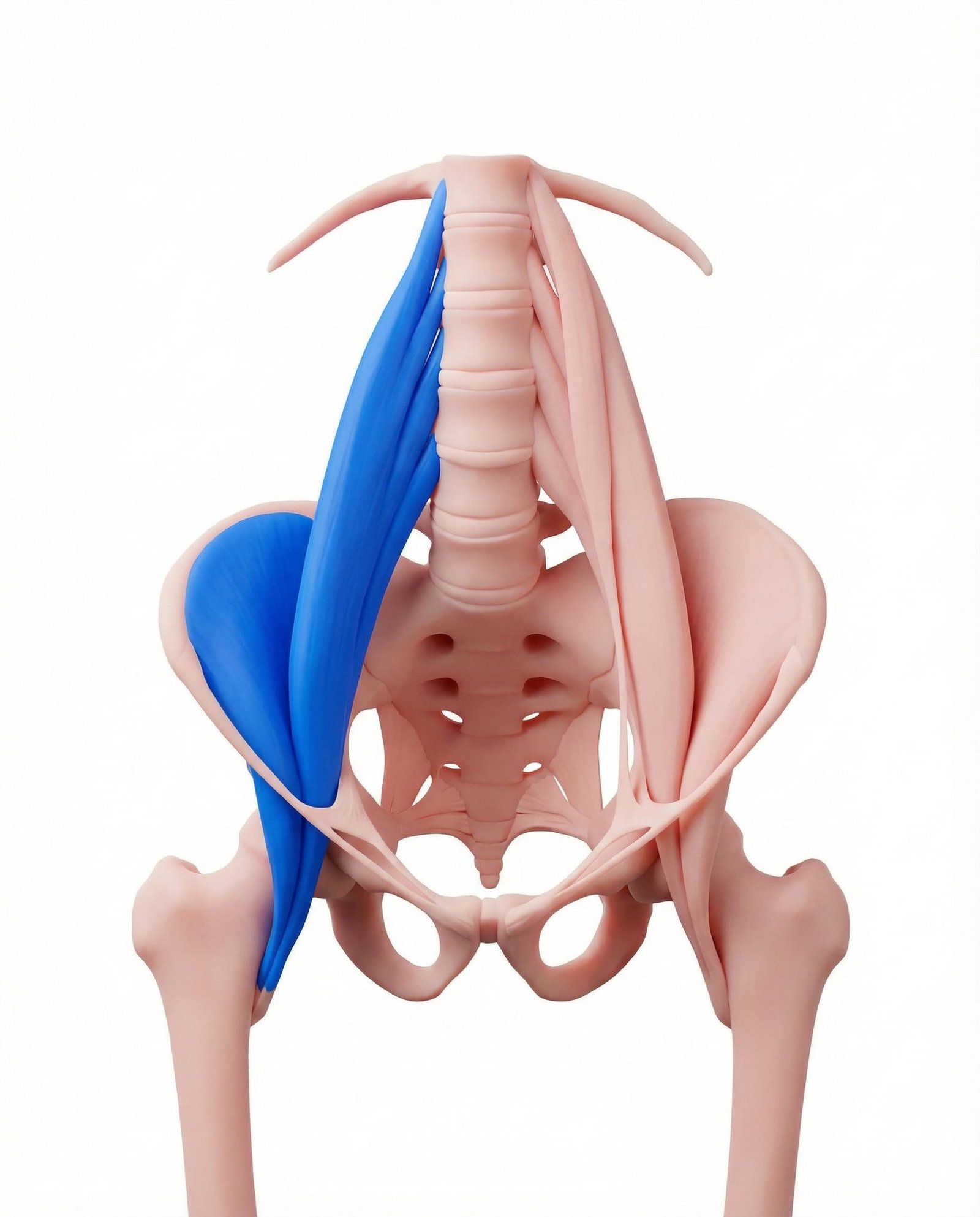
Location. Deep abdomen/pelvis to thigh
Pain referral. Lower back, groin, front of thigh
- Lower back
- Groin
- Front of thigh
- Buttock
Deep lumbar aching from iliopsoas tension increasing anterior pelvic tilt and lordosis
Location. Deep abdomen/pelvis to thigh
Pain referral. Lower back, groin, front of thigh
Location. Iliacus muscle inside the iliac fossa
Pain referral. Groin and medial upper thigh
Location. Lower psoas major near lesser trochanter attachment
Pain referral. Anterior thigh and sacroiliac joint
Lower back pain. Deep lumbar aching from iliopsoas tension increasing anterior pelvic tilt and lordosis
Groin pain. Deep inguinal aching from iliopsoas trigger points near the femoral attachment site
Hip flexor pain. Anterior hip aching worsened by hip extension and prolonged standing activities
Difficulty standing straight. Shortened iliopsoas prevents full hip extension causing forward-leaning trunk posture
Medial thigh ache. Referred pain from iliacus descends to proximal medial thigh along adductor territory
Pain with hip flexion. Active hip flexion contracts iliacus directly loading trigger point within iliac fossa
Difficulty lifting leg. Iliacus trigger point weakens hip flexion force making leg elevation effortful and painful
Groin stiffness in morning. Overnight iliacus shortening with trigger point creates morning hip flexor tightness and groin stiffness
Anterior thigh pain. Lower psoas trigger point refers pain to proximal anterior thigh via femoral nerve pathway
SI joint ache. Psoas tension transmits force to lumbar spine creating compensatory sacroiliac joint strain
Lumbar spine stiffness. Taut lower psoas restricts lumbar extension creating lower back rigidity and stiffness
Difficulty standing upright after sitting. Shortened psoas from sitting resists hip extension making upright posture difficult initially
Hip snapping sensation. Psoas tendon snapping over iliopectineal eminence during hip flexion-extension creates audible click
Prolonged sitting. Sustained hip flexion shortens iliopsoas adaptively creating chronic muscle contracture
Hip flexor overuse. Repetitive hip flexion activities overload iliopsoas beyond its metabolic recovery capacity
Running. Repetitive hip flexion during running stride fatigues iliopsoas with each gait cycle
Weak glutes. Insufficient gluteal strength forces iliopsoas to compensate during hip extension activities
Pregnancy. Increased lumbar lordosis and anterior pelvic tilt during pregnancy overloads the iliopsoas
Stress. Emotional tension activates the psoas as part of the fight-or-flight flexion response
Hip flexor overuse in running. Repetitive hip flexion during running swing phase fatigues iliacus within the iliac fossa
Sit-ups and leg raises. Abdominal exercises demanding hip flexion overload iliacus as primary hip flexor muscle
Soccer and kicking sports. Forceful hip flexion for kicking maximally loads iliacus concentrically exceeding fiber capacity
Post-hip arthroscopy. Surgical trauma to hip joint creates reflex iliacus guarding and post-operative trigger points
Tight hip flexors from sedentary lifestyle. Chronic sitting adaptively shortens iliacus creating trigger points from sustained contracted position
Prolonged sitting with poor posture. Extended seated posture shortens lower psoas at lesser trochanter creating adaptive trigger points
Running and sprinting. Explosive hip flexion during sprinting maximally loads lower psoas at femoral attachment
Martial arts (high kicks). Extreme hip flexion for high kicks overloads lower psoas beyond normal physiological range
Weak gluteal muscles. Gluteal weakness forces psoas to dominate hip extension control creating compensatory overload
Chronic lumbar flexion posture. Sustained lumbar flexion shortens psoas adaptively creating trigger points at lower attachment
Post-surgical hip flexor guarding. Protective hip flexor guarding after surgery creates sustained lower psoas contraction and trigger points
Lie on the edge of a bed with both knees pulled to your chest. Let one leg hang off the edge while holding the other knee. The hanging leg should relax completely, letting gravity stretch the hip flexor. Keep your low back flat against the bed. You should feel a stretch in the front of the hip.
Lie face down with legs straight. Gently lift one leg a few inches off the ground, keeping the knee straight. Hold for 5 seconds, then lower. This gently activates the gluteus maximus while stretching the iliopsoas through reciprocal inhibition.
Kneel on one knee with the other foot flat in front (lunge position). Shift your weight forward, keeping your trunk upright and pelvis tucked under slightly. You should feel a deep stretch in the front of the back hip. For a deeper stretch, raise the arm on the kneeling side overhead and lean slightly to the opposite side.
Lie on your back with knees bent and feet flat. Squeeze your glutes and lift your hips toward the ceiling. Hold at the top for 5 seconds, then lower slowly. This strengthens the gluteus maximus, which is the direct antagonist of the iliopsoas — stronger glutes reduce iliopsoas compensatory overload.
The iliopsoas shortens dramatically during sitting. Stand every 30 minutes and perform a brief hip flexor stretch. Use a standing desk for part of the day. When sleeping, place a pillow under your knees if on your back, or between your knees if on your side, to prevent the hip flexor from shortening overnight.
If groin pain, hip stiffness, or low back pain persists beyond 3-4 weeks, consult a physiatrist. The iliopsoas is deep and often requires professional techniques (such as release through the abdomen or ultrasound-guided injection) for effective treatment. They can also rule out hip joint pathology or inguinal hernia.