TrP 1
TrP1 (Thoracic)
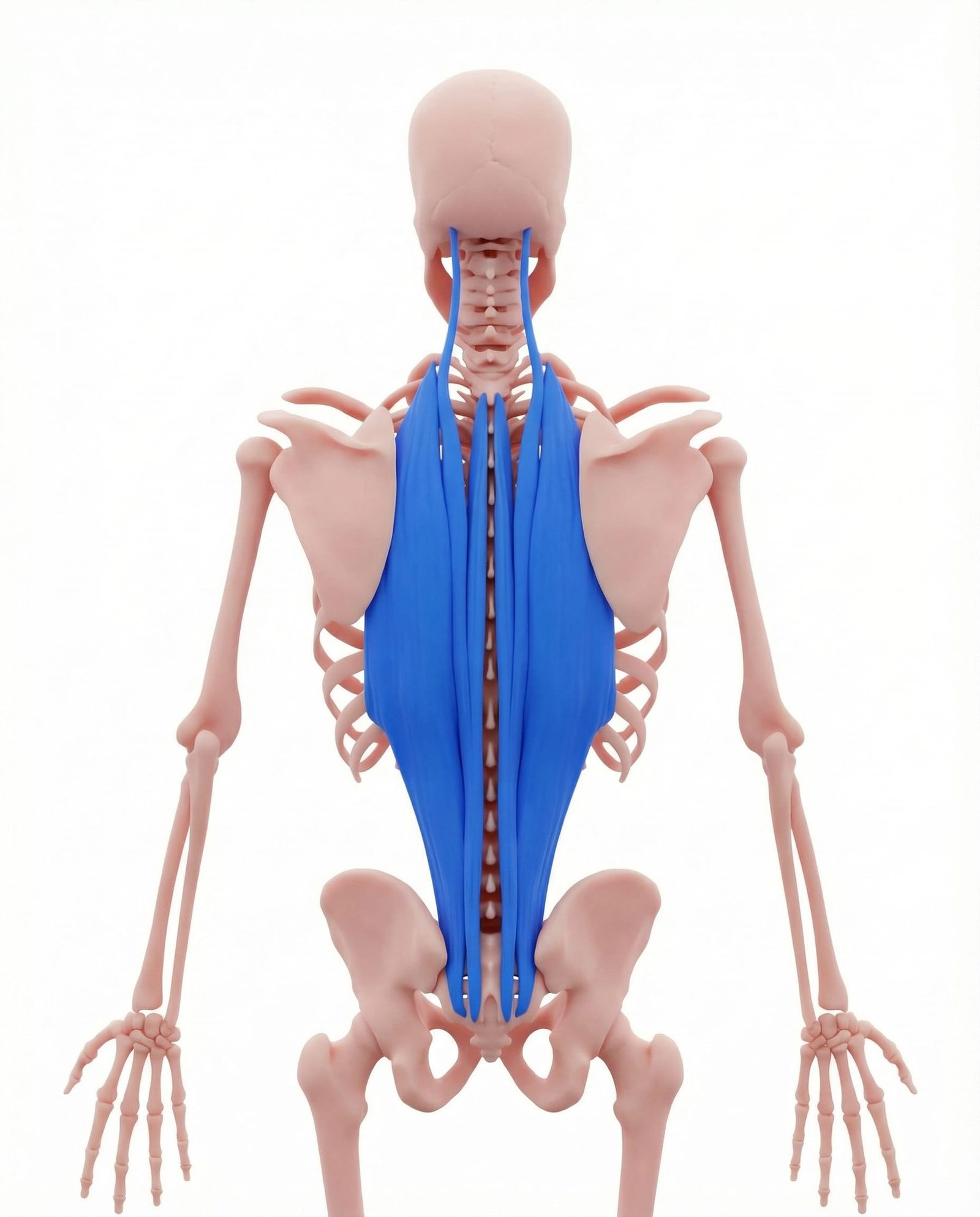
Location. Along thoracic spine
Pain referral. Mid back, along spine
- Mid back
- Along spine
- Rib area
- Abdomen
Paravertebral aching along the thoracic spine worsened by sustained flexed postures
Location. Along thoracic spine
Pain referral. Mid back, along spine
Location. Along lumbar spine
Pain referral. Lower back, buttock, hip
Location. Iliocostalis thoracis, lateral to spine at T6-T9
Pain referral. Lateral mid-back and anterior chest wall
Location. Longissimus thoracis at T10-T12
Pain referral. Lower back and lower abdomen
Location. Iliocostalis lumborum near iliac crest
Pain referral. Buttock and posterior iliac crest
Location. Longissimus lumborum at L3-L5
Pain referral. Deep low back and lower abdominal referral
Mid back pain. Paravertebral aching along the thoracic spine worsened by sustained flexed postures
Spinal tenderness. Localized sensitivity along thoracic spinous processes from erector spinae taut bands
Rib pain. Referred lateral chest wall discomfort from thoracic erector spinae trigger point radiation
Postural ache. Progressive thoracic discomfort developing during prolonged sitting or standing activities
Lower back pain. Bilateral paravertebral lumbar aching that intensifies with prolonged standing or sitting
Spinal stiffness. Restricted lumbar flexion and extension from erector spinae taut band resistance
Pain when bending. Sharp lumbar pain during forward flexion as erector spinae eccentrically controls descent
Morning stiffness. Lumbar rigidity upon waking from sustained recumbent muscle shortening during sleep
Mid-back pain radiating to chest. Iliocostalis referral travels along intercostal nerve pathways to anterior chest wall
Lateral rib aching. Taut bands in iliocostalis thoracis compress and irritate adjacent intercostal structures
Pseudo-cardiac chest pain. Referred pain to anterior chest mimics angina due to shared thoracic dermatomal innervation
Pain with trunk rotation. Rotational movement loads shortened iliocostalis fibers causing ischemic pain provocation
Difficulty with deep breathing. Taut bands restrict rib cage expansion limiting costal excursion during inspiration
Thoracolumbar junction pain. Trigger points at T10-T12 create localized deep aching at the thoracolumbar transitional zone
Lower abdominal ache (referred). Referral follows thoracolumbar nerve pathways projecting pain to the anterior abdominal wall
Pain at beltline. Longissimus fibers at T10-T12 refer pain horizontally at the waistline dermatomal level
Difficulty bending forward. Taut bands in longissimus resist lengthening during trunk flexion causing protective guarding
Stiffness in thoracolumbar transition zone. Sustained contracture at the T10-L2 junction restricts segmental mobility and flexibility
Low back pain radiating to buttock. Iliocostalis lumborum trigger points refer caudally into the ipsilateral upper gluteal region
Pain at iliac crest. Taut bands near the iliac crest attachment create localized periosteal tenderness and aching
Difficulty standing from seated position. Shortened iliocostalis fibers resist the lumbar extension required for sit-to-stand transitions
Unilateral low back ache. Asymmetric trigger point activation produces one-sided paraspinal pain mimicking facet pathology
Stiffness in the morning. Overnight immobility allows trigger point contracture to stiffen requiring gradual warm-up to resolve
Deep low back ache. Longissimus lumborum trigger points at L3-L5 create a deep central paraspinal aching pattern
Lower abdominal discomfort. Referred pain follows lumbar nerve root pathways projecting anteriorly to the abdominal wall
Pain bending and straightening. Taut bands resist both flexion lengthening and extension contraction creating bidirectional pain
Sacral aching. Caudal referral from L3-L5 longissimus projects pain into the sacral and lumbosacral region
Pseudo-visceral lower abdominal symptoms. Somatic referred pain mimics visceral pathology through shared segmental innervation patterns
Poor posture. Sustained thoracic flexion eccentrically overloads erector spinae resisting forward gravitational pull
Prolonged sitting. Extended seated posture fatigues thoracic extensors maintaining upright spinal alignment
Lifting with poor form. Flexion-based lifting transfers excessive load to thoracic erector spinae muscle group
Weak core. Insufficient core stability forces erector spinae to compensate as primary trunk stabilizer
Scoliosis. Lateral curvature creates asymmetric loading on thoracic erector spinae muscle groups
Poor lifting technique. Flexion-based lifting transfers excessive compressive load to lumbar erector spinae fibers
Repetitive bending. Continuous forward bending fatigues lumbar erector spinae beyond metabolic recovery capacity
Obesity. Excess anterior body mass increases lumbar lordosis and erector spinae stabilization demand
Prolonged slouching. Sustained thoracic flexion overloads lateral erector spinae fibers causing ischemic contracture
Heavy lifting with rotation. Combined axial loading and rotation creates shear forces on iliocostalis thoracis fibers
Rowing with excessive trunk rotation. Repetitive rotational torque through thoracic spine overloads lateral paraspinal musculature
Sleeping on one side consistently. Sustained lateral flexion compresses ipsilateral iliocostalis creating chronic ischemic trigger points
Golf and racquet sports. Asymmetric high-velocity trunk rotation generates eccentric overload on contralateral erector spinae
Scoliosis or asymmetric posture. Chronic lateral spinal curvature maintains constant asymmetric loading on thoracic paraspinals
Heavy deadlifting. High axial compressive loads at thoracolumbar junction overload longissimus thoracis fibers eccentrically
Prolonged standing. Sustained antigravity loading fatigues thoracolumbar erector spinae creating ischemic trigger points
Poor seated posture. Excessive lumbar kyphosis shifts mechanical load superiorly to the thoracolumbar junction
Bending and twisting repeatedly. Repetitive combined flexion-rotation movements create cumulative microtrauma in longissimus fibers
Weak core stability. Insufficient transversus abdominis recruitment forces erector spinae to compensate for spinal stabilization
Transitional zone stress from lumbar hyperlordosis. Excessive lumbar lordosis concentrates mechanical stress at the thoracolumbar junction segments
Heavy lifting with poor form. Excessive lumbar flexion under load concentrates strain on iliocostalis lumborum muscle fibers
Gardening and yard work. Prolonged stooped posture with intermittent lifting overloads lumbar iliocostalis eccentrically
Asymmetric loading (carrying child on one hip). Unilateral hip hiking to support load creates sustained contraction in ipsilateral lumbar erectors
Leg length discrepancy. Chronic pelvic obliquity from unequal leg length asymmetrically loads lumbar paraspinal muscles
Weak gluteal muscles. Gluteal insufficiency forces lumbar erectors to compensate during hip extension movements
Chronic poor posture. Habitual lumbar flexion maintains longissimus in a lengthened position causing sustained low-grade strain
Repetitive bending and lifting. Cumulative eccentric-concentric loading cycles create microtrauma in longissimus lumborum fibers
Weak core and gluteal muscles. Inadequate stabilizer support forces longissimus to overwork for both stability and movement
Pregnancy-related postural changes. Anterior weight shift and increased lordosis amplify compressive load on lower lumbar extensors
Tape two tennis balls together or place them in a sock. Lie on your back with the balls positioned on either side of the thoracic spine (not directly on the spine). Gently roll up and down by bending your knees. Hold on tender spots for 20-30 seconds.
Apply a warm, damp towel or heat pack along the mid-back beside the spine. Lie on your back with the heat underneath you. Relax completely and breathe deeply, allowing the warmth to penetrate the deep paraspinal muscles.
Lie on your back with a foam roller positioned across your mid-back. Support your head with your hands. Gently extend backward over the roller, opening up the chest. Hold for a few seconds, then return to neutral. Move the roller up or down one vertebral level and repeat.
Start on all fours. Reach your right arm underneath your body toward the left side, rotating your thoracic spine. Follow your hand with your eyes. Hold for 5 seconds at end range, then reach the same arm up toward the ceiling, rotating the other direction. Repeat on both sides.
Avoid prolonged sitting in one position. Set a timer for every 30 minutes to stand, extend your mid-back gently, and do 3 thoracic rotations to each side. Use a chair with good thoracic support or a lumbar roll to maintain spinal alignment.
If mid-back pain persists beyond 3-4 weeks or if the pain wraps around the ribs, consult a physiatrist. They can evaluate for thoracic disc problems, rib joint dysfunction, or other conditions and provide targeted trigger point treatment.
Lie on your back with both knees bent. Pull one knee toward your chest with both hands, keeping the other foot flat on the floor. Hold for 30 seconds, feeling a gentle stretch in the low back. Switch sides. Then pull both knees to your chest simultaneously.
Apply a warm heat pack or microwaveable pad across the lumbar spine. Lie on your back with the heat underneath you, or recline in a chair with the pack behind your low back. The heat should be comfortably warm, not hot.
Start on all fours with a neutral spine. Extend your right arm forward and left leg backward simultaneously, keeping your back flat and hips level. Hold for 5 seconds, then return to start. Switch to left arm and right leg. Focus on maintaining trunk stability throughout.
Lie on your back with knees bent and feet flat. Gently flatten your low back against the floor by tilting your pelvis backward (tightening your abdominals). Hold for 5 seconds, then relax. This activates the deep core muscles and gently mobilizes the lumbar spine.
Always bend your knees and hinge at the hips when lifting, keeping the object close to your body. Never twist while lifting heavy objects. Use a lumbar support cushion in your chair. Alternate between sitting and standing every 30-45 minutes throughout the day.
If low back pain persists beyond 4-6 weeks of self-care, or if you experience pain shooting down your leg, numbness, or weakness, consult a physiatrist. They can assess for disc herniation, spinal stenosis, or facet syndrome and provide targeted trigger point treatment.