TrP 1
TrP1
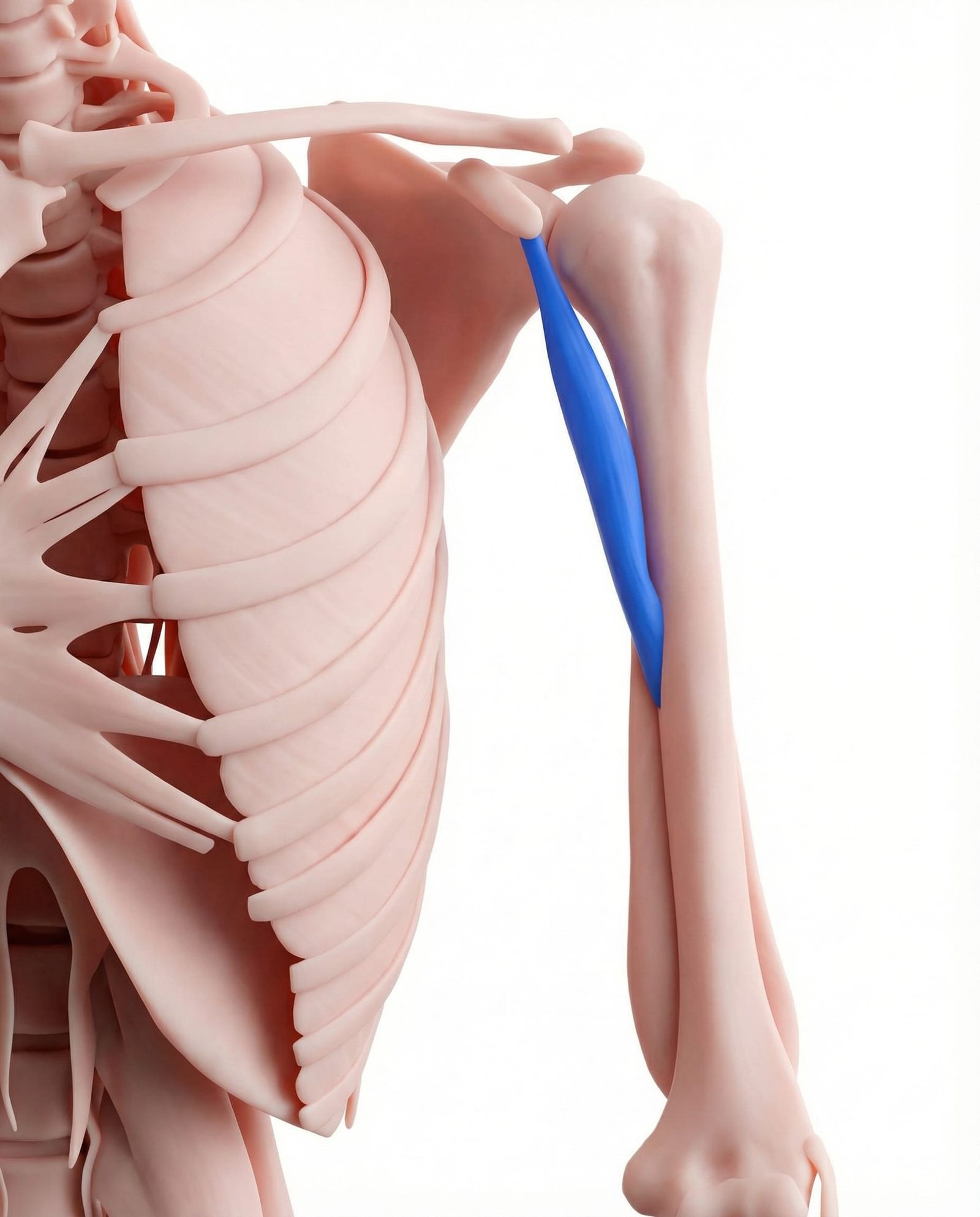
Location. Upper inner arm, deep
Pain referral. Front of shoulder, back of arm
- Front of shoulder
- Back of arm
- Dorsal forearm
Deep anterior shoulder aching near the coracoid process worsened by arm flexion
Location. Upper inner arm, deep
Pain referral. Front of shoulder, back of arm
Location. Inner upper arm
Pain referral. Inner arm, front shoulder
Location. Distal musculotendinous junction at mid-humerus
Pain referral. Medial upper arm and antecubital fossa
Deep shoulder pain. Deep anterior shoulder aching near the coracoid process worsened by arm flexion
Arm pain. Referred ache down posterior arm and dorsal forearm from coracobrachialis trigger points
Difficulty with flexion and adduction. Pain limiting combined shoulder flexion and adduction movements like reaching across body
Inner arm pain. Medial upper arm aching from coracobrachialis trigger points along inner humeral shaft
Shoulder discomfort. Anterior shoulder pain from coracobrachialis trigger point referral to coracoid process area
Forearm ache. Distal referral extending to dorsal forearm from coracobrachialis trigger point activation
Medial upper arm aching. Distal coracobrachialis trigger points create medial upper arm aching along the bicipital groove
Pain at inner elbow region. Referral extends distally to the antecubital fossa and medial elbow joint region
Difficulty with full elbow extension. Coracobrachialis trigger points create referred tension limiting comfortable full elbow extension
Medial arm pain when reaching forward. Forward reaching demands coracobrachialis shoulder flexion provoking distal trigger point referral
Anterior forearm tightness. Distal referral extends into the proximal anterior forearm creating perceived tightness
Rock climbing. Sustained pulling with shoulder flexion and adduction overloads coracobrachialis during climbing
Pull-ups. Repeated shoulder adduction under body weight fatigues coracobrachialis muscle fibers chronically
Gymnastics. Complex shoulder stabilization demands during apparatus work stress coracobrachialis repeatedly
Overhead activities. Prolonged arm elevation requires coracobrachialis stabilization of the glenohumeral joint
Swimming. Repetitive pulling strokes with shoulder adduction fatigue coracobrachialis each stroke cycle
Pulling. Repetitive pulling movements requiring shoulder flexion and adduction overload coracobrachialis fibers
Climbing. Sustained pulling and reaching during climbing overloads coracobrachialis shoulder stabilizer function
Overhead work. Prolonged overhead arm positions create sustained coracobrachialis loading for shoulder stabilization
Repetitive reaching and pushing motions. Sustained forward reaching demands coracobrachialis activation for shoulder flexion and adduction
Bench press with narrow grip. Narrow grip bench press increases coracobrachialis demand for shoulder adduction during pressing
Carrying heavy objects with arms extended. Holding heavy objects at arm length maximally loads the coracobrachialis isometrically
Pull-up exercises. Pull-ups demand coracobrachialis activation for shoulder adduction during vertical pulling
Sustained arm elevation (holding phone overhead). Prolonged arm elevation fatigues the coracobrachialis as a shoulder flexion stabilizer
Stand in a doorway with your affected arm raised to the side and your elbow bent to 90 degrees. Place your forearm and palm flat against the door frame. Step forward through the doorway with one foot until you feel a deep stretch across the front of your shoulder and into the inner upper arm. The coracobrachialis shares its attachment point with the pectoralis minor at the coracoid process, so this stretch effectively targets both muscles. Keep your shoulder blade pulled back and down to maximize the stretch on the coracobrachialis.
Sit with your affected arm resting at your side, slightly away from your body with the palm facing forward to expose the inner arm. Using the thumb and fingers of your opposite hand, gently grasp the inner upper arm between the biceps and triceps muscles. Press your thumb into the inner arm tissue, starting near the armpit and working downward toward the mid-arm. When you find a tender spot, hold steady pressure for 20-30 seconds. Be gentle in this area as the neurovascular bundle runs nearby.
Stand with a light resistance band anchored behind you at waist height. Hold the band in the affected hand with your arm at your side. Slowly bring your arm forward and slightly across your body (combining flexion with adduction), which is the primary action of the coracobrachialis. Control the return to the starting position over 3 seconds. Start with very light resistance and focus on smooth, controlled movement. You should feel the inner upper arm muscles engage without sharp pain.
Stand with your back flat against a wall, feet about 12 inches from the wall. Press your head, upper back, and buttocks against the wall. Raise your arms to shoulder height with elbows bent at 90 degrees, pressing the backs of your hands and forearms against the wall. Slowly slide your arms up the wall toward an overhead position while maintaining contact with the wall, then slide them back down. The movement should be slow and controlled. If you cannot maintain wall contact, reduce the range of motion.
Throughout the day, focus on keeping your shoulders gently pulled back and down rather than allowing them to round forward. Set a reminder every 30-60 minutes to check your posture and reset. When sitting, ensure your chair supports your lower back so your thoracic spine stays upright. When standing, imagine a string pulling the top of your head toward the ceiling. Avoid crossing your arms in front of your body for prolonged periods as this shortens the coracobrachialis. Consider using a posture reminder device or app during the initial correction period.
If inner arm pain with hand or finger symptoms persists beyond 3-4 weeks of self-care, consult a physician or physical therapist experienced in upper extremity conditions. A professional can differentiate coracobrachialis trigger points from thoracic outlet syndrome, brachial plexus compression, or cervical radiculopathy through specific clinical tests including the EAST test, Adson test, and neural tension tests. They may perform targeted manual release of the coracobrachialis, which is difficult to self-treat due to its deep location near the neurovascular bundle.
Sit with the affected arm resting at your side, palm facing forward. Using the thumb of your opposite hand, press into the inner aspect of the upper arm, roughly midway between the armpit and the elbow. The coracobrachialis lies deep to the biceps, so you will need to press through the biceps muscle to reach it. Search for the most tender spot and apply sustained pressure for 30-60 seconds. Breathe slowly and allow the pressure to gradually reduce the tenderness. Move to any adjacent tender spots.
Stand in a doorway with the affected arm raised to shoulder height and the forearm resting against the door frame, elbow bent at 90 degrees. Step forward through the doorway with the leg on the same side, allowing your body to rotate away from the arm until you feel a comfortable stretch across the front of the shoulder and inner arm. Hold for 30 seconds. Repeat 3 times. For additional stretch of the coracobrachialis specifically, extend the arm further back with the palm facing up.
Lie face down on a bench or the edge of a bed with the affected arm hanging straight down, holding a light weight (2-3 pounds). Keeping the arm straight, slowly raise it out to the side until it is level with your body, squeezing the shoulder blade. Hold for 2 seconds, then lower over 3 seconds. Perform 10-12 repetitions for 3 sets. This strengthens the posterior shoulder muscles that oppose the coracobrachialis, restoring muscular balance.
Stand with the affected arm at your side. Place a folded towel or small pillow between your upper arm and your torso. Gently squeeze the towel against your body using shoulder adduction force, holding for 10 seconds. Release for 5 seconds. Repeat 10 times. Next, with your arm still at your side, press your palm forward against a wall using gentle shoulder flexion force, holding for 10 seconds, 10 repetitions. These isometric exercises strengthen the coracobrachialis without stressing it through range.
Temporarily reduce or modify activities that heavily load the coracobrachialis — climbing, pull-ups, swimming (especially breaststroke and butterfly), and carrying heavy objects close to the body. When carrying items, hold them with arms slightly away from the body rather than pressed against the torso. Avoid prolonged reaching across the body. During workouts, warm up the shoulder thoroughly and avoid sudden increases in pulling volume. Sleep with a pillow supporting the arm to prevent it from falling across the chest.
If deep inner arm pain persists beyond 3-4 weeks despite self-care, consult a sports medicine physician or physical therapist experienced with shoulder and upper extremity myofascial pain. They can differentiate coracobrachialis trigger points from musculocutaneous nerve entrapment, biceps pathology, or shoulder labral tears. Treatment may include targeted dry needling, instrument-assisted soft tissue mobilization, or manual therapy addressing the coracobrachialis and associated shoulder girdle muscles.