The Basics

Myofascial Pain Syndrome Overview
The core concept:
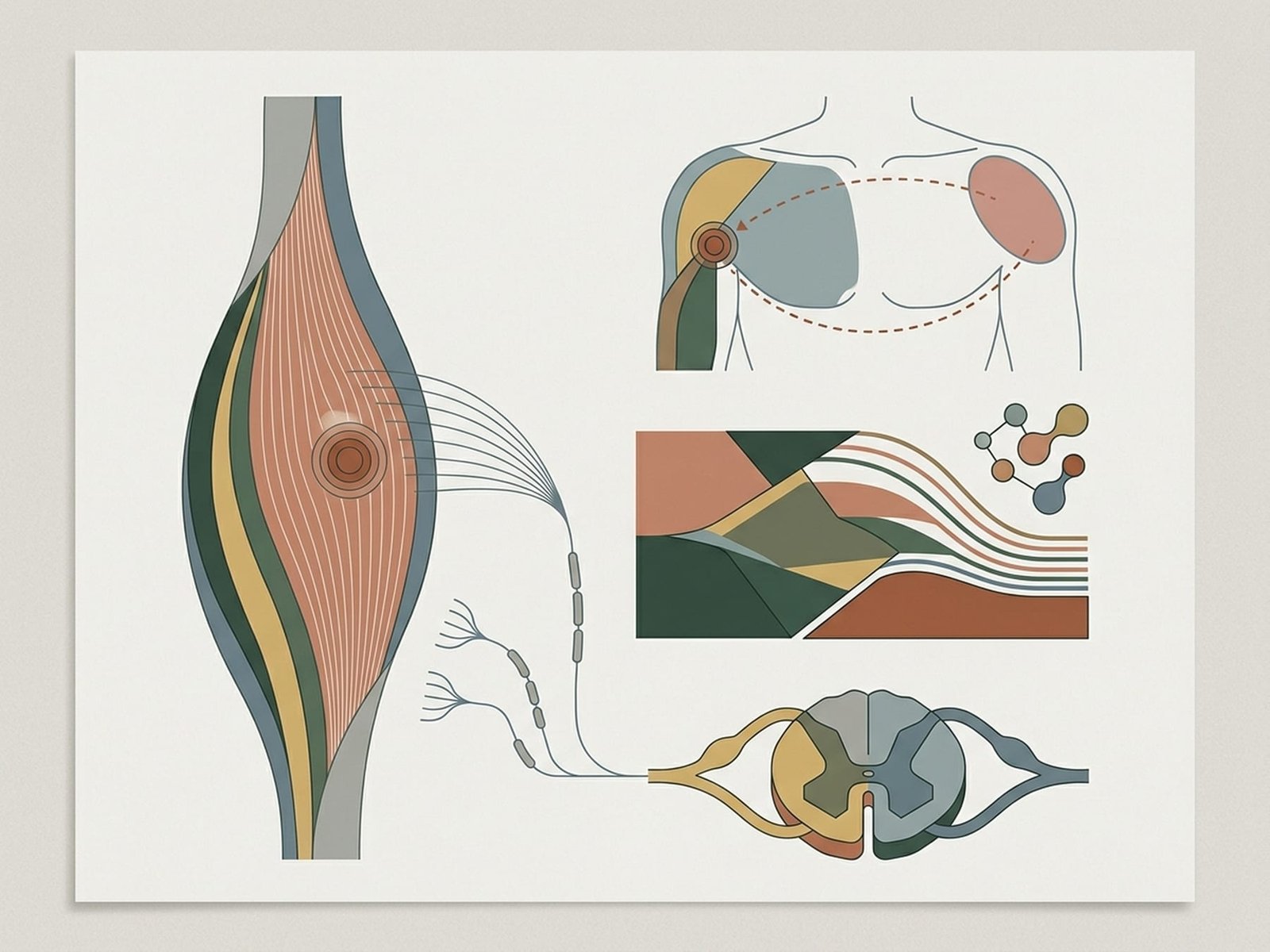
Muscles can develop tight, irritable areas called trigger points. These points are tender when pressed and may send pain to other parts of the body in recognizable patterns. This is called referred pain, and it is one of the main reasons the condition can feel confusing or “misplaced.”
Myofascial pain syndrome is a common contributor to musculoskeletal pain, but it is not always assessed routinely in general practice.
For example, a trigger point in the neck may contribute to headache. A trigger point in the upper back may create pain felt in the front of the shoulder. A trigger point deep in the hip may create a pain pattern that resembles sciatica.
Because the painful area and the actual source may not match, imaging and testing focused only on the painful area may not explain the symptoms well.
The word “myofascial” refers to both muscle and the connective tissue around it. In practice, MPS is usually understood as a muscle-centered pain pattern with associated soft-tissue involvement and referred pain behavior.
When to consider myofascial pain
MPS may be worth considering when pain persists without a clear structural explanation, when symptoms and imaging do not match well, or when a repeatable referred pain pattern is present. It is not the explanation for all unexplained pain, but it is a recognized and clinically useful possibility.
How It May Feel
Common descriptions from people with myofascial pain
A deep ache that persists
Often not a sharp, stabbing sensation, but more like a dull, deep ache inside the muscle. Rest may reduce it temporarily, but the pain often returns with activity, posture, or stress.
Pain that seems to move or spread
The source of the pain and the place where you feel it are not always the same. This is one reason MPS can feel confusing and hard to localize.
Morning stiffness
Many people feel stiff on waking and then loosen up with movement. The stiffness may return later in the day after prolonged sitting, stress, or overuse.
A tender spot in the muscle
There may be a focal area in the muscle — sometimes described as a knot or tight band — that is especially tender. Pressing it may reproduce a familiar pain pattern.
Pain that worsens with stress
Stress does not necessarily create trigger points by itself, but it often increases muscle tension, pain sensitivity, and symptom intensity.
Tingling or altered sensation
Some patients report tingling, numbness, or odd sensations near painful muscles. These symptoms can overlap with nerve-related conditions, which is why proper clinical assessment matters.
If these descriptions sound familiar
This does not prove that you have MPS, but it can be a reasonable reason to seek a hands-on musculoskeletal evaluation — especially if your symptoms have been hard to explain.
Could This Be Relevant to Me?
A brief checklist — not a diagnosis
If several of these sound familiar, it may be worth discussing myofascial pain with a clinician who evaluates musculoskeletal pain patterns directly.
Pressing a specific spot reproduces a familiar pain — sometimes in a different area.
Your pain tends to recur in the same area or follow the same general pattern.
Stretching, movement, or warmth helps temporarily, but symptoms return.
Your pain began after overuse, injury, poor sleep, or a period of stress or tension.
Stress, poor sleep, prolonged posture, or cold exposure seem to make it worse.
Imaging has not identified a clear structural explanation that fully matches the symptoms.
Massage or focused pressure gives at least temporary relief.
You can feel tender, firm, or ropey areas in the affected muscle.
The symptom pattern feels real and repeatable, but hard to explain with one simple diagnosis.
MPS and Other Conditions
How MPS relates to conditions it is sometimes confused with

Trigger Point vs Tender Point Comparison
MPS can mimic, overlap with, or coexist with other diagnoses. A diagnosis of arthritis, fibromyalgia, neuropathy, or stress-related tension does not automatically exclude a myofascial component.
MPS vs. Fibromyalgia
What Is Similar
- Both can involve muscle pain, tenderness, fatigue, and poor sleep
- Stress can worsen symptoms in both
- Both may feel chronic and difficult to explain at first
What Is Different
- MPS is usually more regional and tied to specific muscles or trigger points
- Fibromyalgia is typically more widespread and more centrally amplified
- MPS often responds better to localized physical treatment than fibromyalgia alone
Can They Coexist?
Yes. The two can coexist. In those cases, addressing the myofascial component may still reduce the overall symptom burden, even if it does not resolve the whole pain picture.
MPS vs. Arthritis
What Is Similar
- Both can cause pain, stiffness, and movement limitation
- Both can affect similar body regions
- Both may feel worse after inactivity
What Is Different
- Arthritis is primarily a joint problem; MPS is primarily a muscle and soft-tissue problem
- Arthritis is often visible on imaging; MPS usually is not
- MPS often produces referred pain patterns that do not line up neatly with one joint
Can They Coexist?
Yes. Painful joints often lead to secondary muscle guarding and trigger points nearby, so both processes may be present at once.
MPS vs. Nerve Damage (Neuropathy)
What Is Similar
- Both may produce pain, tingling, numbness, or burning symptoms
- Both can be difficult to localize precisely
- Both may feel as if they travel down an arm or leg
What Is Different
- Neuropathy tends to follow more recognizable nerve distributions
- MPS follows muscle and referral patterns rather than classic nerve maps
- Nerve damage is more likely to show measurable neurological findings or testing changes
Can They Coexist?
Yes. Trigger points can irritate nearby nerves, and nerve problems can create muscular overload or guarding. Sorting them out requires examination, not assumption.
MPS vs. Stress-Related Muscle Tension
What Is Similar
- Stress can increase both muscle tension and pain intensity
- Both may cause neck, shoulder, or jaw discomfort
- Both may improve with relaxation and better sleep
What Is Different
- MPS usually includes more focal and reproducible physical findings
- Ordinary stress tension may ease more fully when the stressor changes
- Trigger point patterns are typically more consistent and more mechanically reproducible
Can They Coexist?
Yes. Stress is one of the most common perpetuating factors in MPS. The presence of a stress component does not make the physical findings less real.
Myofascial Pain Syndrome Mechanism
Why Is This Not Better Known?
Why awareness is still inconsistent
Myofascial pain is well described in the literature, but awareness and comfort with diagnosis vary widely. Several practical reasons help explain that:
It is diagnosed mainly by examination
Trigger points are primarily identified through history and palpation, not through imaging or standard blood work. In settings that rely heavily on scans and labs, that can make MPS easier to overlook.
Training varies
Not all clinicians receive the same depth of training in trigger point examination, referred pain patterns, or musculoskeletal palpation. This is a training issue, not proof that the condition is imaginary.
It overlaps with many better-known diagnoses
Because MPS can resemble headaches, radiculopathy, TMJ disorders, low back pain syndromes, or tendon problems, it may be considered only later in the process.
Stress can complicate interpretation
Stress is a real perpetuating factor in MPS, but that can sometimes lead people to underweight the physical findings. Stress and real muscle pain can coexist.
Coding and research history have been inconsistent
Historically, MPS has not always been tracked or studied as consistently as more imaging-visible or lab-test-supported diagnoses.
If this has been a long road
Many people with MPS describe a long period of uncertainty before the pattern is recognized. That reflects the diagnostic challenge — not a failure of credibility on the patient’s part.
Treatment Options
Several approaches may help, often in combination
MPS can improve with treatment, especially when trigger points are identified and the factors keeping them active are addressed. The speed and extent of recovery vary significantly between people.
Manual Therapy
Hands-on work such as trigger point pressure release, soft-tissue treatment, and myofascial techniques can help reduce local pain and improve movement tolerance.
Dry Needling
Some patients improve with dry needling, particularly in clearly localized trigger point patterns. The strength of evidence varies by region and technique.
Self-Care Techniques
Heat, stretching, pressure tools, and movement-based self-care often help reduce day-to-day symptom burden and complement professional treatment.
Addressing Contributing Factors
Sleep, posture, ergonomics, movement habits, stress, and nutritional issues are often part of the treatment plan because they can strongly influence recurrence.
What Recovery May Look Like
Recent, localized trigger points
Newer and more localized cases often improve faster than long-standing ones, especially when the main aggravating factor is identified early.
Longstanding or recurrent trigger points
Chronic cases usually need more time, more consistency, and more attention to the habits or conditions that keep the pain recurring.
General expectations
Progress is usually gradual rather than dramatic. Some people improve quickly; others improve in stages as the load pattern, sleep, stress, and movement quality improve.
Trigger Point Formation Process
Common Trigger Points
Six frequently discussed muscles and their typical referral patterns
Upper Trapezius
Top of the shoulder / base of the neck
Typical Referral Area
Up the side of the neck and into the temple
How It May Present
May feel like a tension-type headache with shoulder tightness. Many people instinctively massage this area when the headache starts.
Masseter
Jaw muscle
Typical Referral Area
Teeth, ear, eyebrow, and side of the face
How It May Present
Can feel like dental pain or jaw pain. It is a common contributor to clenching- and TMJ-related symptom patterns.
Infraspinatus
Back of the shoulder blade
Typical Referral Area
Deep ache in the front of the shoulder and upper arm
How It May Present
Often confusing because the pain is felt in front, while the source is behind the shoulder.
Quadratus Lumborum (QL)
Deep lower back between ribs and pelvis
Typical Referral Area
Lower back, hip, buttock, and sometimes around the side of the abdomen
How It May Present
Often a deep one-sided low back ache that worsens with prolonged standing, bending, or twisting.
Piriformis
Deep buttock
Typical Referral Area
Buttock pain with possible radiation down the back of the thigh
How It May Present
May resemble sciatica, especially when sitting aggravates it. Clinical assessment is important to separate it from nerve-root pain.
Gastrocnemius
Calf muscle
Typical Referral Area
Back of the knee, arch, or underside of the foot
How It May Present
May show up as calf tightness, night cramps, arch pain, or vague pain behind the knee rather than just “calf pain.”
Explore trigger points by body region
Select a body region to explore common muscles and trigger points associated with that area and the places they may refer pain.
What Can Contribute to Trigger Points?
Common influences on trigger point development and persistence
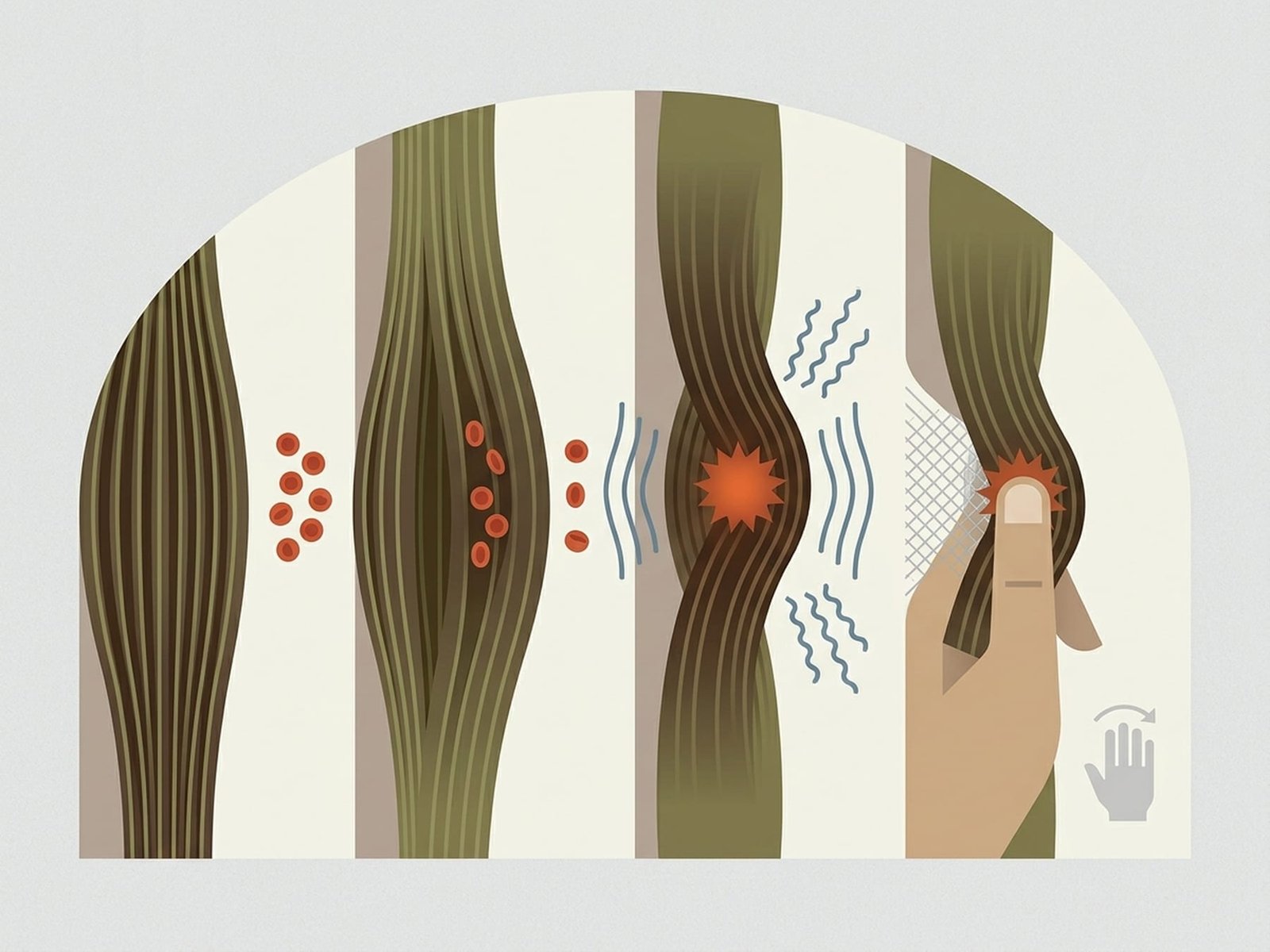
Trigger points usually do not arise “out of nowhere.” They tend to appear when muscles are overloaded, strained, deconditioned, held too long in one position, or recovering poorly.
Prolonged static postures
Posture
Long periods in the same position — especially desk work, driving, or phone posture — can keep certain muscles under sustained low-level load.
Overuse or sudden load changes
Activity
A sudden increase in activity, repetitive movement, or doing more than the muscle is prepared for can contribute to trigger point development.
Stress and muscle bracing
Stress
Stress often shows up physically as jaw clenching, shoulder elevation, shallow breathing, and chronic muscle tension.
Injury or trauma
Injury
Falls, accidents, sports injuries, and protective guarding after injury can all leave muscles irritable long after the initial event.
Sleep quality and sleep position
Sleep
Poor sleep or a sleep position that strains the neck, jaw, shoulder, or back can make muscular pain harder to settle.
Nutritional factors
Nutrition
In some patients, deficiencies such as vitamin D, B12, magnesium, or iron may increase muscle irritability or slow recovery.
An important point
Developing trigger points does not mean you failed your body. They are a common response to everyday mechanical, emotional, and recovery-related stressors. The real question is what keeps them active once they appear.

MPS Diagnostic Criteria
Muscle Overload
Injury, repetition, sustained tension, or deconditioning may overload parts of a muscle.
Local Irritability
A focal region may become unusually sensitive, tense, and harder to relax normally.
Pain Sensitization
The local area becomes more pain-responsive and may start to influence nearby movement patterns.
Referred Pain
Pain may be felt away from the source, which is one reason the pattern is easy to misread.
Next Steps
Reasonable places to go from here
If this page sounds familiar, the next step is usually not self-diagnosis — it is better pattern recognition and a more targeted conversation with the right clinician.
Self-Assessment Tool
A guided questionnaire to help you organize whether trigger points may be relevant to your symptoms.
Start assessment
Talking to Your Doctor
A practical guide to discussing musculoskeletal pain clearly and productively with your clinician.
Read the guide
Body Map
Explore common muscles and trigger point referral patterns by body region.
Open body map
Frequently Asked Questions
Answers to common questions about trigger points and myofascial pain.
Browse questions
Treatment Overview
A practical overview of self-care, professional treatment, and what treatment usually aims to achieve.
View treatments
Where to go from here
A careful hands-on examination remains the best way to determine whether trigger points are contributing to your symptoms. Learning the pattern is a useful first step; confirming it clinically is the next one.
Understanding the pattern can make the path to evaluation and treatment much clearer.