What Is TENS?

T E N S Treatment
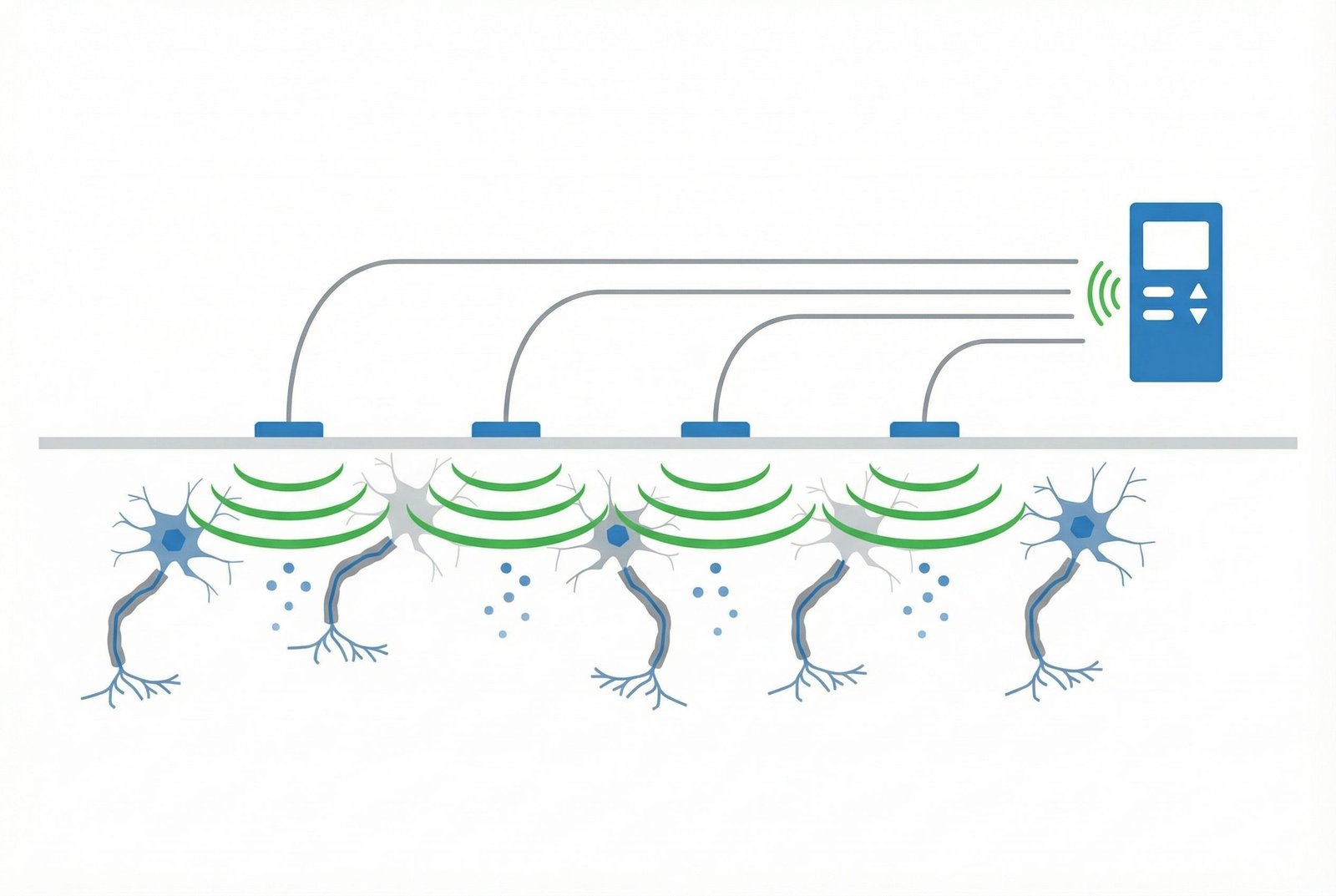
Overview DiagramTranscutaneous Electrical Nerve Stimulation (TENS) uses low-voltage current delivered through surface electrodes placed on the skin. It is one of the most accessible electrotherapy options available for home use.
In myofascial pain, TENS is best thought of as a symptom-management tool. It can reduce pain, improve movement tolerance, and make stretching or exercise easier, but it should not be framed as a direct cure for the trigger point itself.
TENS is best understood as a low-risk pain-modulation tool that can create a more comfortable window for active treatment.
That is why TENS is most useful as part of a broader plan that also includes active rehabilitation, self-care, and — when appropriate — more targeted clinical treatment.
Mechanism of Action
Several mechanisms are proposed for TENS. The most important practical point is that it modulates pain rather than directly remodeling the trigger point itself.
Mechanism of Action
Mechanism DiagramGate Control Theory
Endogenous Opioid-Related Effects
Descending Inhibitory Pathways
Reduced Peripheral Irritability
Central Sensitization Support
Limits in Trigger Point Treatment
TENS Modes & Parameters
Different TENS modes feel different and may suit different patients or situations. Comfort, practicality, and repeatability often matter as much as theoretical mechanism.
Conventional (High-Frequency) TENS
Often 80–120 HzPulse Often short pulse widths
MechanismMost commonly explained through segmental pain-modulation mechanisms such as gate-control effects, where non-painful sensory input competes with pain signaling.
- — Usually feels like buzzing, tingling, or electrical vibration under the electrodes
- — Typically used at a sensory rather than motor level
- — Can be useful while working, moving, or doing daily tasks
- — Often chosen first because it is easier to tolerate
- — Some users notice reduced benefit over time if settings never change
Best for:Short-term symptom relief during activity or daily life. Often the most practical first mode to try.
Acupuncture-Like (Low-Frequency) TENS
Often low frequencyPulse Often longer pulse widths
MechanismOften described as engaging broader pain-modulation systems, including endogenous opioid-related pathways and descending inhibition.
- — Usually produces visible or noticeable muscle twitching
- — May feel less comfortable than conventional TENS
- — Often used as a session-based treatment rather than worn casually through the day
- — Some patients prefer it when standard sensory TENS feels too brief
- — Tolerability varies a lot between individuals
Best for:Dedicated treatment sessions when a stronger but slower-building effect is acceptable.
Burst Mode TENS
High-frequency pulses delivered in low-frequency burstsPulse Device-dependent
MechanismOften described as combining some of the features of conventional and low-frequency TENS in one mode.
- — Usually feels rhythmic rather than continuously buzzing
- — Can be easier to tolerate than sustained low-frequency twitching
- — May be worth trying if standard high-frequency TENS plateaus
- — Often available on mid-range consumer devices
- — Works best when settings are individualized rather than copied blindly
Best for:A reasonable compromise when the patient wants a stronger effect than conventional TENS but better tolerance than pure low-frequency stimulation.
Modulated / Random TENS
Automatically varies within a programmed rangePulse Automatically varies depending on the device
MechanismThe main rationale is reducing accommodation by varying the stimulation pattern rather than keeping it identical throughout the session.
- — Settings change automatically during use
- — May reduce the sense that the body is getting used to the stimulation
- — Useful when long sessions are part of the strategy
- — Common on many consumer units
- — Not automatically superior, but often worth testing
Best for:Longer sessions where the patient feels standard TENS tends to “fade out.”
Interferential Current (IFC)
Medium-frequency carrier currents creating a lower-frequency beat patternPulse Not expressed in the same way as standard TENS
MechanismThe main idea is that medium-frequency current passes the skin more comfortably, allowing treatment of deeper tissues through a beat frequency generated in the field.
- — Usually uses a four-electrode setup
- — Often better suited to clinic equipment than simple home units
- — May feel more comfortable than strong low-frequency TENS at similar depth goals
- — Often used for broader or deeper regions rather than a single superficial trigger point
- — Best understood as a clinical electrotherapy option rather than a standard consumer tool
Best for:Selected deeper pain regions, usually in clinical settings rather than routine home use.
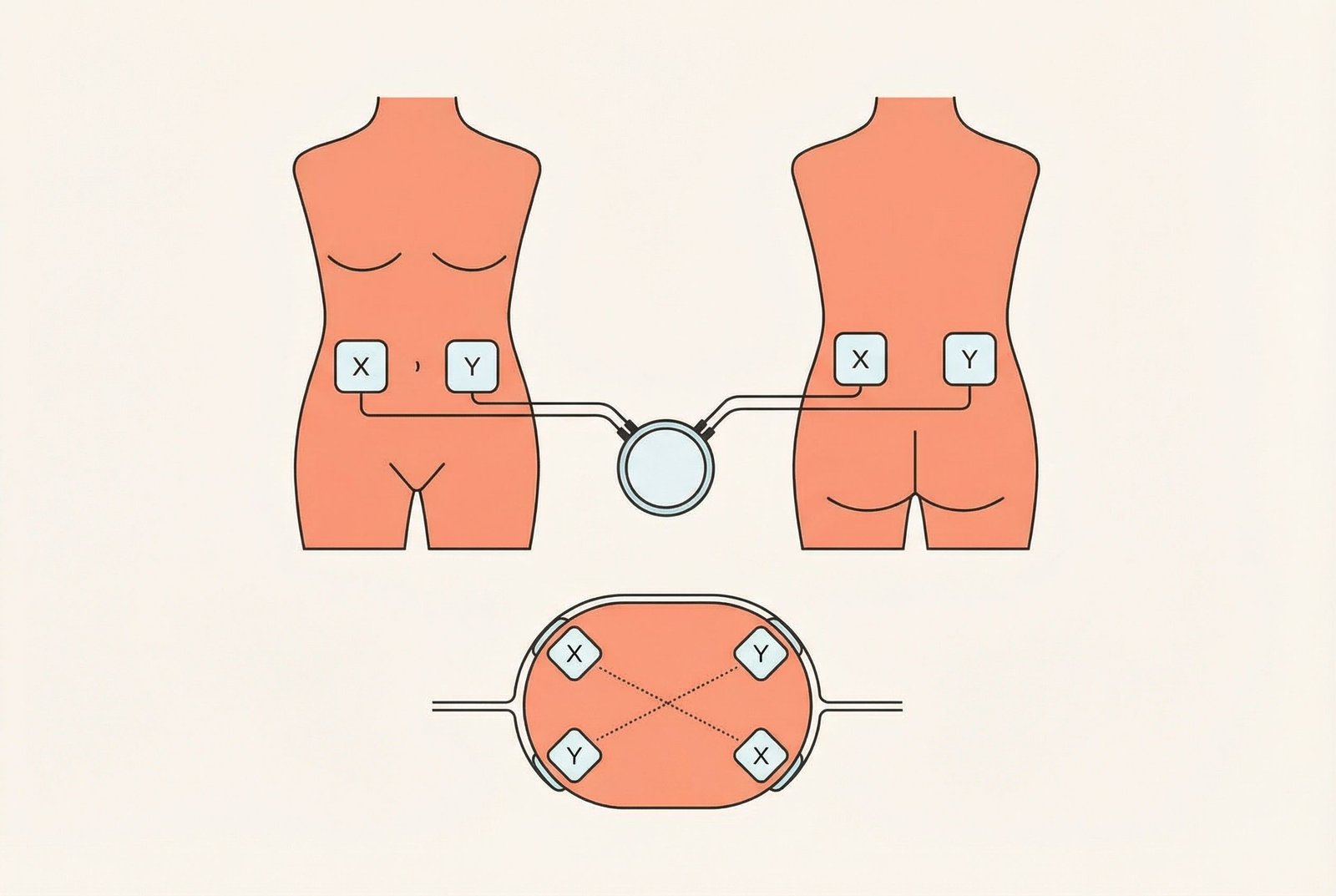
Electrode Placement for Trigger Point Pain
Electrode placement should be guided by anatomy, comfort, and symptom reproduction — not by overly rigid formulas. Simple placements are often the best starting point.
Direct Trigger Point Placement
Electrodes are placed over or around the region of the palpable trigger point. This is often the simplest and most intuitive first approach.
When to UseA good first option when the trigger point location is clear and the local tissue tolerates electrodes well.
- — Place the electrodes so the target area sits between or beneath the stimulation field
- — Smaller electrodes can improve precision in focal regions
- — Adjust the spacing if the current feels too superficial or too diffuse
Surrounding / Bracketing Placement
Electrodes are arranged around the painful region rather than placed directly on one exact point. This is often useful when pain is broader or there are several nearby active spots.
When to UseUseful for diffuse trigger point regions, larger muscles, or when direct placement is too uncomfortable.
- — Try to let the main current path cross the painful region
- — A two-channel setup can be useful in broader muscles
- — This is often a better option than repeatedly chasing one exact tender point
Dermatomal / Referred Pain Placement
Electrodes are placed over the region where the patient actually feels the pain, even if the trigger point itself is somewhere else.
When to UseUseful when the referred pain is the main complaint, such as temple pain from upper-trapezius or SCM-related patterns.
- — Map the referred pain pattern carefully first
- — This can be combined with direct trigger point placement using another channel
- — Use it when treating the “felt pain” is more practical than treating the hidden source immediately
Segmental / Paravertebral Placement
Electrodes are placed near the spinal segments that correspond to the painful region. The goal is to influence pain modulation more proximally rather than only at the trigger point itself.
When to UseSometimes useful in chronic or widespread cases, or when direct placement is too sensitive or impractical.
- — Keep the placement anatomically sensible rather than overly theoretical
- — This works best when the clinician understands the pain distribution and segmental logic
- — Use it as one option, not as a mandatory advanced strategy
Motor Point Stimulation
Electrodes are placed where stimulation most easily recruits the target muscle. This is more relevant when using stronger, twitch-producing modes.
When to UseWhen the treatment goal includes muscle contraction, local pumping, or more active neuromuscular input.
- — Use this more cautiously than simple sensory TENS
- — The “right” point is usually the one that produces useful contraction with the least current
- — This approach is more technique-sensitive than basic sensory placement
Common Placement Examples by Muscle
Common Placement Examples by Muscle
- Upper Trapezius — Place electrodes over the upper trapezius belly, usually bracketing the most irritable portion of the muscle. A second channel can be added if the painful area is broad or extends into the neck.
- Infraspinatus — Place electrodes across the infraspinous fossa so the painful posterior cuff region sits within the stimulation field. If the main complaint is anterior referred pain, a second channel can sometimes be added more distally.
- Levator Scapulae — A common approach is to place one electrode near the angle of the neck and another toward the superior scapular angle to cover the length of the muscle.
- Quadratus Lumborum — Because the QL is deep, surface TENS often works better as a broader regional treatment rather than a precise “trigger point” treatment. Larger electrodes and wider spacing may be more practical here.
- Suboccipital Muscles — Small electrodes at the base of the skull may be useful in selected cervicogenic headache patterns, provided placement is comfortable and safe. Intensity is usually kept conservative in this area.
Clinical Evidence
Johnson & Martinson (2007)
Vance et al. (2014)
Clinical Guideline Context
Early Myofascial Trigger Point Studies
Comparative Work
Consensus Summary
Safety Profile
Pain Reduction
Accessibility
How to Use TENS at Home
The biggest advantage of TENS is that patients can try it repeatedly at home and decide whether it helps enough to stay in the plan.
How to Use TENS at Home
Step-by-Step IllustrationSelect a Reasonable Device
Prepare the Skin
Position the Electrodes
Start Low and Increase Gradually
Use Reasonable Session Lengths
Change Parameters When Needed
Maintain the Electrodes
Pair TENS With Active Care
Safety Precautions & Contraindications
TENS vs Other Electrotherapies
TENS is one of several electrotherapy options. Its strengths are accessibility, safety, and ease of self-use rather than depth or precision.
TENS
PENS
Electroacupuncture
Interferential Current (IFC)
Therapeutic Ultrasound
Limitations of TENS for Myofascial Pain
TENS can be very useful, but only when the patient understands what it can and cannot do.
Does Not Directly Resolve the Trigger Point
Tolerance / Accommodation
Limited Depth of Penetration
Mixed Evidence Base
Highly Individual Response
Usually Requires Repeated Use
Sensory Competition
Non-painful electrical input may compete with pain signaling while the unit is on.
Descending Modulation
Some settings may engage broader pain-inhibitory systems beyond the local segment.
Movement Tolerance
Reduced pain can make stretching or exercise easier to perform.
Short-Term Relief
TENS is best thought of as creating a temporary treatment window rather than fixing the tissue itself.
TENS is a safe, non-invasive option for reducing pain and making movement or treatment more tolerable in some myofascial pain patients.
Its main role is symptom modulation, not direct trigger point resolution.
Conventional high-frequency TENS is often the easiest place to start because it is usually the most comfortable and practical.
Electrode placement matters, but simple, anatomically sensible placement usually works better than overcomplicated rules.
TENS tends to work best when paired with stretching, exercise, self-myofascial release, or rehabilitation rather than used as a stand-alone solution.
A reasonable home trial is often worthwhile because the response is highly individual.
The best TENS plan is one that the patient can tolerate, repeat, and integrate into active recovery.
TENS is most useful when patients understand both its value and its limits.
The Bottom LineTENS is a useful low-risk adjunct for myofascial pain, especially when the goal is to reduce pain enough to move, stretch, work, or sleep more comfortably. It is most effective when it helps the patient do something active afterward, not when it becomes the entire plan.