The “You Are Not Alone” Numbers
Chronic pain can feel isolating, but myofascial pain is widely encountered in both the general population and pain clinics. These numbers are best understood as estimates that vary by population and diagnostic method.
Curiosities
Overview IllustrationThe “Wait, That’s Connected?” Files
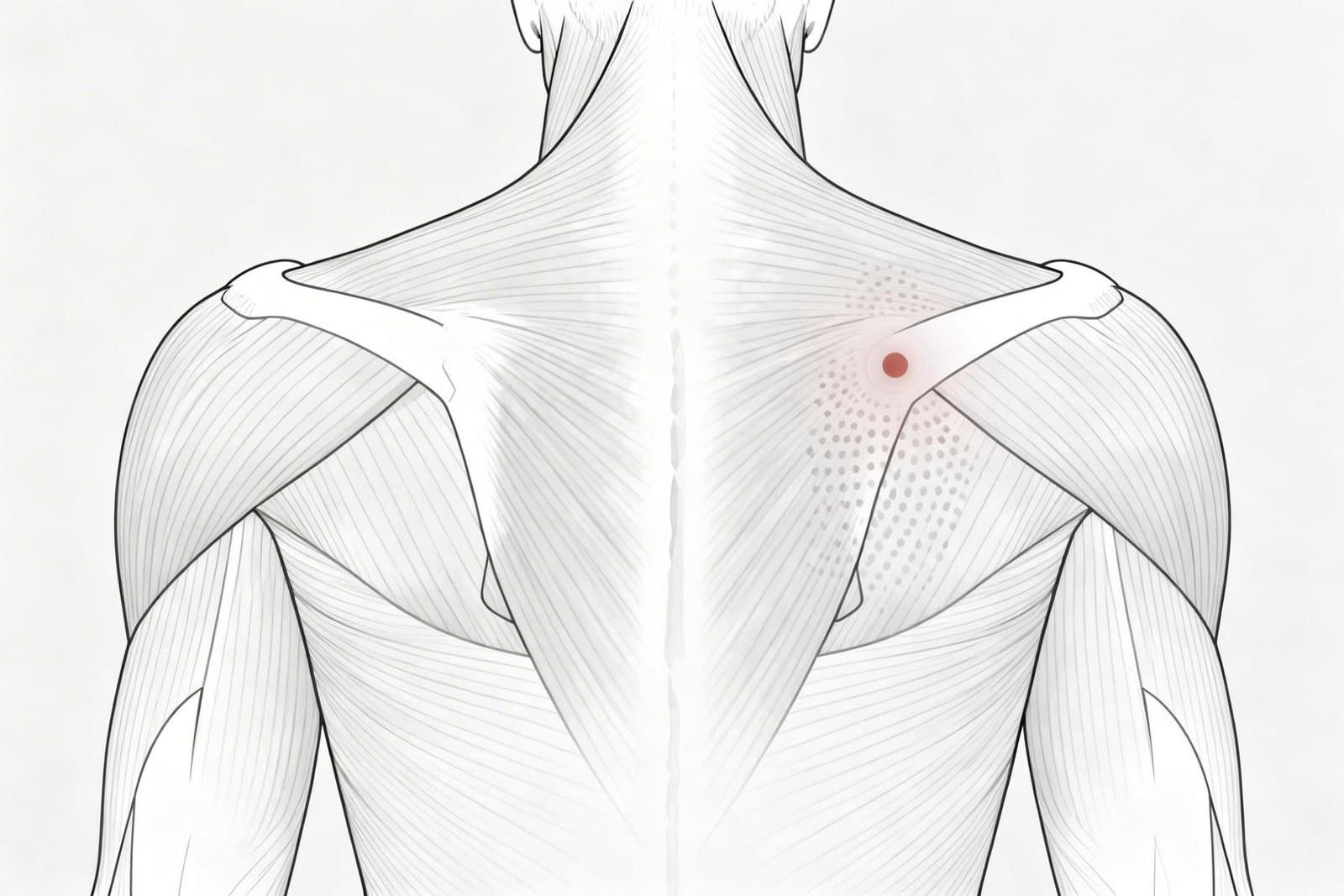
Trigger points can create referred pain in locations that seem unrelated to the source muscle. This is one reason myofascial pain can be so misleading in practice.
One of the most clinically surprising features of myofascial pain is that the place that hurts is not always the place generating the problem.
The Great Pretender
Sternocleidomastoid (SCM)
This neck muscle is well known in trigger point literature for producing a broad and sometimes confusing symptom pattern. SCM symptoms can overlap with ENT, jaw, or cervical complaints and often lead to diagnostic confusion.
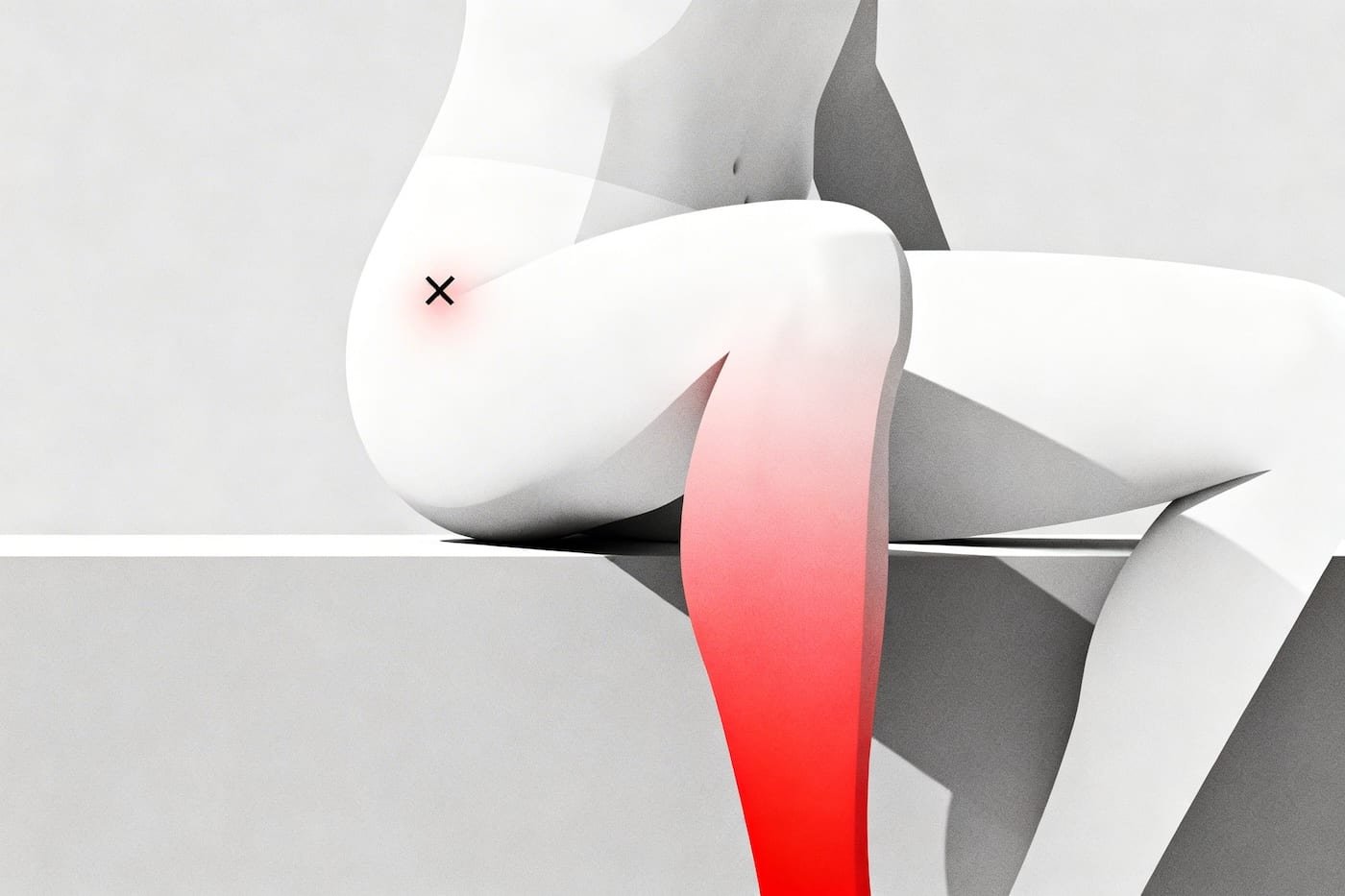
The Fake Sciatica
Gluteus Minimus
Trigger points in the gluteus minimus can create a striking leg-pain pattern that may resemble radicular or sciatic pain. It is not identical to nerve-root sciatica, but it is one of the classic myofascial mimics.
The Dental Decoy
Masseter
The masseter can refer pain into the teeth and jaw in a way that may be mistaken for primary dental pathology. This is one reason persistent tooth pain with a negative dental workup sometimes deserves a muscular exam.
The Wrist Mystery
Subscapularis
This deep shoulder muscle can send pain surprisingly far down the arm. Its referred pattern is one of the better examples of why a local wrist complaint is not always generated at the wrist.
The Chest Impersonator
Pectoralis Minor
Pectoralis minor symptoms can overlap with chest or upper-quarter pain patterns that feel alarming to patients. It should never replace cardiac evaluation when red flags are present, but it is a real musculoskeletal mimic in selected cases.
The Ear Deceiver
Lateral Pterygoid
Deep jaw muscles can refer pain toward the ear region and may coexist with TMJ-related symptoms. In some cases the ear itself is normal, while the pain source is musculoskeletal.
The Belly Faker
Abdominal Obliques
Abdominal wall trigger points can create symptoms that overlap with visceral pain. They are not the explanation for every abdominal complaint, but they are an important differential when organ-based causes have not explained the full picture.
Fascinating Body Quirks
Some of the stranger and more clinically interesting ways trigger points may interact with the nervous system and movement control.
Curiosities
The "Jump Sign"
When a particularly irritable trigger point is pressed, patients may flinch, withdraw, or vocalize unexpectedly. This “jump sign” is a familiar clinical observation and can support the impression that a point is highly reactive.
The Local Twitch Response
During needling or snap palpation, a small visible or palpable twitch may occur within the affected muscle. Clinicians often treat this as a useful sign that the dysfunctional region has been engaged, though it is not the sole determinant of treatment success.
System Overload (Autonomic Phenomena)
Trigger points do not always produce pain alone. In some regions, especially the head, jaw, and neck, they may be associated with tearing, sweating, goosebumps, or other autonomic-like responses that seem disproportionate to a muscle problem.
The Domino Effect (Satellite Points)
Longstanding pain in one region may alter movement and load in another, and secondary “satellite” trigger points may develop. This is one reason treating only the most painful area sometimes gives incomplete relief.
Active vs. Latent Points
Some trigger points are active and reproduce the patient’s familiar pain. Others are latent — tender and dysfunctional, but not spontaneously painful day to day. Latent points can still matter because they may restrict movement or become active under stress or overload.
Referred Pain Patterns
Referred pain remains one of the most clinically important features of trigger points. It explains why treatment directed only at the place that hurts can sometimes miss the actual source muscle.
Proprioception Sabotage
Active trigger points may interfere with motor control and body-position sense. Some studies suggest patients with active trigger points show reduced proprioceptive accuracy or altered balance, especially in the neck and shoulder region.
The Sleep Reactivation Cycle
Many patients report waking stiffer or more painful than when they went to bed. Prolonged static positions during sleep, local compression, and reduced movement overnight may contribute to this pattern in susceptible muscles.
Bilateral Mirroring
Pain and sensitivity patterns can sometimes appear on both sides of the body even when the original overload seemed one-sided. This may reflect compensation, bilateral muscle use, or broader sensitization rather than a simple one-muscle problem.
A Brief, Wild History
From traditional point-based treatment systems to presidential medicine to modern imaging methods, the history of myofascial pain is full of unusual turns.
Ancient Accords
Traditional Chinese Medicine has long described tender therapeutic points, including “Ah Shi” points. The phrase is often translated roughly as “Yes, that’s it” or “That’s the spot,” which is one reason it is frequently compared with modern trigger point ideas.
Coining the Term
Dr. Janet Travell helped popularize the phrase “trigger point” in the 20th century as she developed the modern clinical language around referred muscular pain.
Presidential Treatment
President John F. Kennedy was treated for chronic pain by Dr. Janet Travell, who later became the first female Physician to the President. Her work helped bring trigger point concepts into wider medical attention.
The Lewit Observation
Karel Lewit’s work helped show that dry needling could produce relief comparable to injectate-based approaches in some cases. This shifted attention toward the mechanical and neurophysiological effect of the needle itself.
Shah’s Discovery
Dr. Jay Shah and colleagues used microdialysis techniques to study the biochemical environment of active trigger points and reported differences in pH and inflammatory or neuroactive substances compared with normal muscle.
Seeing is Believing
Ultrasound and elastography studies have helped visualize regional stiffness differences in muscle that may correspond to trigger point zones. These techniques do not solve every diagnostic question, but they made the topic harder to dismiss as purely subjective.
Treatment Oddities: How We Fix It
Some myofascial treatments seem counterintuitive at first, yet make more sense when you look at the underlying clinical logic.
Curiosities
Treatment Oddities: How We Fix ItThe Dirty Sponge Effect
Sustained Pressure
Sustained pressure can feel counterintuitive because it briefly compresses an already painful area. Clinically, the goal is to change local tissue tension and sometimes improve the way the region feels once the pressure is released. The “sponge” analogy is memorable, even if the physiology is more complex than a simple flush-in/flush-out model.
Dry Needling
No Medication Needed
A very thin needle inserted into a trigger point may reduce pain even without medication. Proposed explanations include mechanical disruption, altered motor endplate activity, local twitch response, and broader spinal pain-modulation effects.
The Paradox of "Good Pain"
Post-Treatment Soreness
After successful treatment, the muscle may feel sore for 24 to 48 hours. This does not automatically prove the treatment worked, but mild short-term soreness is common and often represents a manageable post-treatment response rather than a treatment failure.
Spray and Stretch
Vapocoolant Therapy
Cooling the skin briefly with a vapocoolant spray may reduce guarding and discomfort enough to allow a more tolerable stretch. Historically this was a classic Travell-era technique, although it is used less routinely today.
Ultrasound Elastography Visualization
Seeing the Invisible
Advanced imaging can sometimes show localized stiffness differences in muscle that correspond to clinically identified trigger point regions. This does not turn trigger point diagnosis into a pure imaging problem, but it adds useful support to the clinical model.
The ESWT Regenerative Paradox
Breaking to Heal
Shockwave therapy is thought to work partly by creating a controlled biological stimulus that may alter pain sensitivity, tissue turnover, and local healing behavior. It is better described as a targeted mechanical stimulus than as a simple “break it to fix it” intervention.
Did You Know?
Curious clinical and scientific facts about trigger points, muscle pain, and why the body can behave so strangely.
Trigger Points Can Stay Quiet for Long Periods
Latent trigger points may remain relatively silent for long periods and then become symptomatic during stress, overload, illness, poor sleep, or abrupt changes in movement patterns.
Muscles May Become More Re-Irritable
A previously symptomatic muscle may become painful again more easily under repeated overload or poor recovery, especially if the original perpetuating factors were never fully addressed.
The Weather Connection
Many patients report symptom changes with weather shifts, especially cold, damp conditions or barometric pressure changes. The exact mechanism is still debated, but the observation is common enough that it deserves to be taken seriously without overstating certainty.
Emotional Connections
Stress and emotional load can influence muscle tension, sleep, breathing pattern, and pain sensitivity. This is one reason regions such as the upper trapezius and jaw muscles often flare during stressful periods.
The 60-90 Second Rule
Many clinicians hold sustained trigger point pressure somewhere in the 30-90 second range, sometimes longer, depending on tolerance and the technique being used. There is no universal magic threshold, but very brief pressure often does less than intended.
Exercise May Calm Trigger Points Over Time
Regular, appropriate exercise may reduce myofascial pain vulnerability by improving circulation, load tolerance, conditioning, and stress regulation. The key is appropriate dosage, since overloading too early can do the opposite.
The 400+ Map
Travell and Simons described a very large number of referred pain patterns across many muscles. Their work remains one of the most influential clinical atlases in myofascial pain medicine, even though not every pattern carries identical evidentiary weight.
Why Understanding the Pattern Helps
Understanding the logic behind pain patterns can reduce fear and help patients make better sense of confusing symptoms. Knowing that a wrist ache can originate in the subscapularis, or tooth pain in the masseter, changes which exam a patient asks for.
A condition that felt random becomes more manageable once the referral patterns and treatment options are visible.